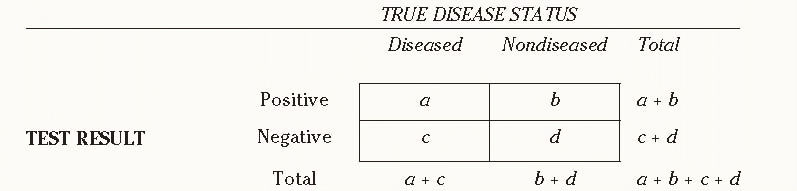
asymptomatic disease, while diagnostic tests are obtained in symptomatic patients. A positive screening result in an individual rarely provides direct evidence of disease; screening tests must be followed by diagnostic tests to determine whether disease is truly present.
for image archiving. Full-field digital mammography (FFDM), in comparison to SFM, has been shown to have lower noise, higher contrast, and improved dynamic range (4). In addition, FFDM allows immediate display of digital images on a monitor without film processing, enabling more rapid interpretation (5). Moreover, FFDM makes the use of computeraided detection (CAD) software, which recognize suspicious image patterns, a possibility.
TABLE 10-1 Standard 2 × 2 Table Comparing Test Results and Disease Status of Subjects Tested, along with Formulas to Measure Test Characteristics | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||
a small reduction in breast cancer mortality from screening (65). However, the reduction did not reach statistical significance. Thus, the effectiveness of routinely screening women 40 to 49 years of age remains controversial, with concern regarding whether or not the magnitude of benefit from routine screening sufficiently outweighs the harms of false positives and overdiagnosis.
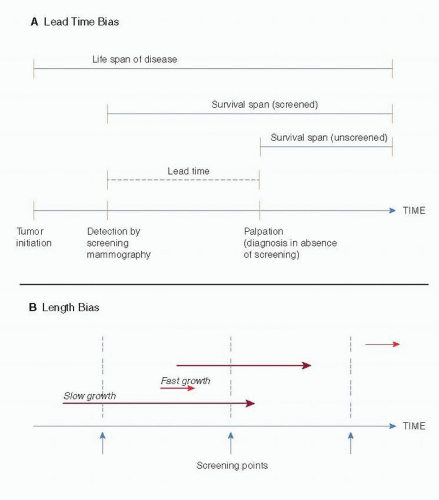 FIGURE 10-1 Lead-time (A) and length (B) bias. In part B, the length of the arrows represents the time required for the tumor to reach a palpable size. (From Institute of Medicine (IOM). Mammography and beyond: developing technologies for the early detection of breast cancer: a non-technical summary. The National Academies Press. http://www. nap.edu/openbook.php?record_id=10107&page=7) |
geographic units designed to be heterogeneous with regards to urban versus rural, population size, and socioeconomic factors. Women with preexisting breast cancer were excluded from both groups. This trial enrolled approximately 80,000 women to screening and just over 39,000 women in the control group from Ostergotland, Sweden, and approximately 39,000 women to screening and 18,000 in the control group from Kopparberg, Sweden. The intervention included one-view mammography every 2 years for women younger than 50 years and every 33 months for women 50 years and older. Contamination was much lower in this study compared to other RCTs; approximately 13% had mammograms as part of routine care, mostly in the later years of the study. The relative risk of breast cancer death for the screened population in the study was reported as 0.82 (0.64-1.05) in Ostergotland and 0.68 (0.52-0.89) in Kopparberg. Concerns have been raised about the randomization methods used as well as the analysis, which required correction for late performance of the control group mammography. However, the group from Sweden has performed subsequent meta-analysis that addressed many of these questions (70, 71, 74, 75 and 76).
Related posts:
 Pathology of Benign Breast Disorders
Pathology of Benign Breast Disorders
 Ductal Carcinoma In Situ and Microinvasive Carcinoma
Ductal Carcinoma In Situ and Microinvasive Carcinoma
 Adjuvant Systemic Therapy: Endocrine Therapy
Adjuvant Systemic Therapy: Endocrine Therapy
 Preoperative Endocrine Therapy for Operable Breast Cancer
Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Preoperative Endocrine Therapy for Operable Breast Cancer
Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


