Bone Lesions
Felasfa M. Wodajo
Osteoma
Osteoma of bone is a densely mineralized endosteal lesion almost always seen in the head. The most common locations are in the ethmoid and frontal sinuses. The lesions are uniformly benign and usually discovered incidentally. In unusual cases, very large osteomas of the paranasal sinuses can cause obstruction of the nasal air ducts or other cranial symptoms. The radiographic hallmark is dense, ivory-like mineralization with smooth margins. Unless there are obstructive symptoms, observation is appropriate.
Pathogenesis
Etiology
Unknown
Component of Gardner’s syndrome
Epidemiology
Estimated prevalence: 0.4%
Male:female ratio: 2:1
Location: ethmoid and frontal sinuses of the cranium most common
Pathophysiology
Osteomas are benign, indolent lesions.
Capacity for slow growth but no malignant potential
Diagnosis (See Algorithm 5.1-1)
Clinical Features
Typically incidental findings on dental or other cranial radiography
Occasionally, very large osteomas cause sinus obstruction, loss of smell, or even in rare cases invasion into intracranial structures.
Radiographic Features
Plain radiographs and computed tomography (CT): smooth-contoured, densely mineralized lesion, within the medullary bone with no cortical invasion
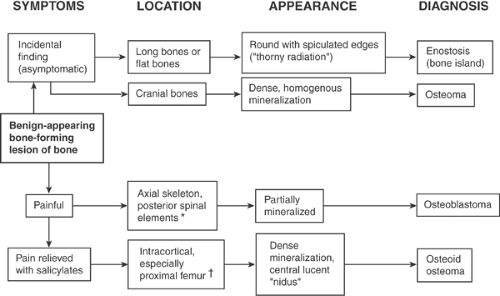 Algorithm 5.1-1. Diagnosis of benign-appearing bone-forming lesions of bone. *Most common;may also occur in long bones, but rarely. †Most common;may also occur in posterior spinal elements and flat bone. |
Histologic Features
Mature lamellar bone with decreased marrow component
Sometimes haversian canals are seen within areas resembling cortical, compact bone.
Differential Diagnosis
Cemento-ossifying Fibroma (Ossifying Fibroma of Craniofacial Bones)
This is also another ossifying lesion of the cranium, but more often found in the mandible than the maxilla and cranial bones.
It must be distinguished from osteoma as it may have a more aggressive course and more often requires excision.
It appears as a well-circumscribed ossifying matrix, occasionally with expansile remodeling.
In contrast to dense ossification of osteoma, the periphery of these lesions is not always completely mineralized.
The histological appearance is also different, showing a mix of fibrous and fibromyxoid stroma in addition to combination of woven and lamellar bone and sometimes cementum.
Osteoid Osteoma
These have been described in the head and neck and also appear as small, densely mineralized lesions but with the important difference of a central radiolucent nidus and often nocturnal pain relieved by salicylates, in contrast to incidental, asymptomatic osteoma.
Chronic Sclerosing Osteomyelitis
Low-grade bone infections, presumably of oral origin, occur in the maxilla and mandible and appear as sclerotic lesions but are usually discovered due to symptoms.
Parosteal Osteosarcoma
A rare juxta-cortical variant of osteoma, parosteal osteoma, is sometimes confused with parosteal osteosarcoma.
The distinguishing feature of parosteal osteoma is the presence of dense, homogenous mineralization, whereas the mineralization in parosteal osteosarcoma may be incomplete and heterogeneous.
Treatment
Surgical Treatment
Surgical intervention is rare as the vast majority of osteomas are asymptomatic, incidental findings.
Excision has been occasionally reported for rare lesions with obstructive symptoms of the sinuses.
Results and Outcome (Prognosis)
Observed lesions may progress very slowly.
Enostosis
Enostosis or “bone island” is a small, asymptomatic, densely mineralized lesion found within the cancellous bone. It is typically an incidental finding; the important diagnostic challenge often is ruling out the possibility of the lesion representing a small bone metastasis. The characteristic radiating thick trabeculae seen on imaging studies and absence of uptake on bone scan are distinguishing features.
Pathogenesis
Etiology is unknown.
Epidemiology
Most often found in adults undergoing testing for other reasons, although presumably develops at a younger age during skeletal maturation
No gender predilection or inheritance pattern
Distribution
Found within cancellous bone
Preference for pelvis, femur, and other long bones
Relatively rare in the spine
Pathophysiology
Disorder of endochondral ossification
An error in resorption of the secondary spongiosum during bone formation leads to an island of heavily calcified matrix left within the spongy, cancellous bone.
Enostoses do not change in size over time and have no malignant potential.
Diagnosis (See Algorithm 5.1-1)
Clinical Features
Asymptomatic, incidental findings, usually discovered during evaluation for other reasons
Radiologic Features
Radiographs
Round or ovoid, homogeneously dense, sclerotic focus in cancellous bone
Distinctive finding is the presence of radiating bony streaks (“thorny radiation”) emanating from the sclerotic center.
Almost always small, ranging from 1 mm to 2 cm
“Giant” bone islands, measuring up to 6 cm, have been reported, but large lesions should raise suspicion for other diagnoses.
Computed Tomography/Magnetic Resonance Imaging
Distinctive “brush borders” are more clearly seen on CT and are diagnostic.
Appearance on magnetic resonance imaging (MRI) examination should emulate cortical bone.
Bone Scan
Most important radiographic feature of enostosis is the usual absence of uptake on bone scan, which—when present—differentiates it from metastatic disease.
Occasional scintigraphically active enostoses have been described, suggesting caution in using bone scan as the only modality for diagnosis, but bone scan remains very important in diagnosis.
Histologic Features
Features include mature lamellar pattern with haversian canals within a focus of compact (cortical) bone.
Thickened, radiating trabeculae merge with the surrounding trabeculae in the periphery of the lesion (Fig. 5.1-1).
Differential Diagnosis
Metastasis
Differentiating enostosis from bone metastases is the most important diagnostic challenge.
Small blastic lesions can be seen in breast cancer and prostate cancer metastases.
Metastases usually show increased uptake on bone scan.
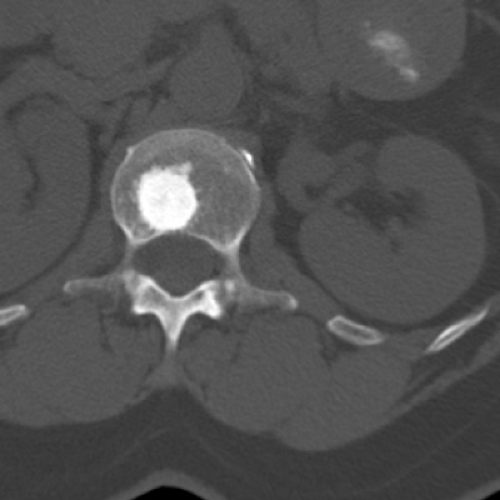 Figure 5.1-1 Enostosis in vertebral body. Note dense mineralization and thickened, radiating trabeculae. |
Osteopoikilosis
Osteopoikilosis is an inherited autosomal dominant disorder in which numerous enostoses are found, usually at the ends of long bones.
Similar to isolated enostosis, no uptake is seen on bone scan.
Osteopetrosis (Albers-Schönberg Disease)
This is typically a polyostotic disorder caused by an error in resorption of the primary spongiosum.
The hallmark is dense osteosclerosis filling the entire medullary canal, as opposed to isolated bone islands.
Enchondroma
A small enchondroma may be difficult to distinguish from an enostosis.
CT imaging should help distinguish the pattern of mineralization.
Enchondromas demonstrate incomplete mineralization with a speckled or whorled pattern in contrast to the dense, homogenous mineralization of enostoses.
Enchondromas almost always demonstrate uptake on bone scan.
Treatment
Surgical Treatment
No surgery is indicated; the main role of the consulting surgeon is to exclude other diagnostic possibilities.
Prognosis
Observed lesions rarely progress.
Osteoid Osteoma
Osteoid osteoma is a small, painful bone lesion that most commonly occurs in the cortices of long bones, with a prediction for the proximal femur. The pain pattern is usually distinctive, with nightly pain rapidly alleviated with salicylates (aspirin). The lesion has a characteristic small, radiolucent central nidus measuring up to 1 to 2 cm and thick, surrounding reactive bone. Standard treatment is percutaneous radiofrequency ablation.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


