Adrenal myelolipomas are benign, hormonally inactive neoplasms composed of myeloid elements and mature adipose tissue in varying proportions. Unilateral adrenal myelolipomas are uncommon (see Case 65), and bilateral adrenal myelolipomas are even more uncommon and usually associated with chronic corticotropin (ACTH) hypersecretion. The most common clinical setting of bilateral adrenal myelolipomas is untreated or poorly treated congenital adrenal hyperplasia (CAH). Herein we share such a case and additional examples of the findings on computed tomography (CT).
Case Report
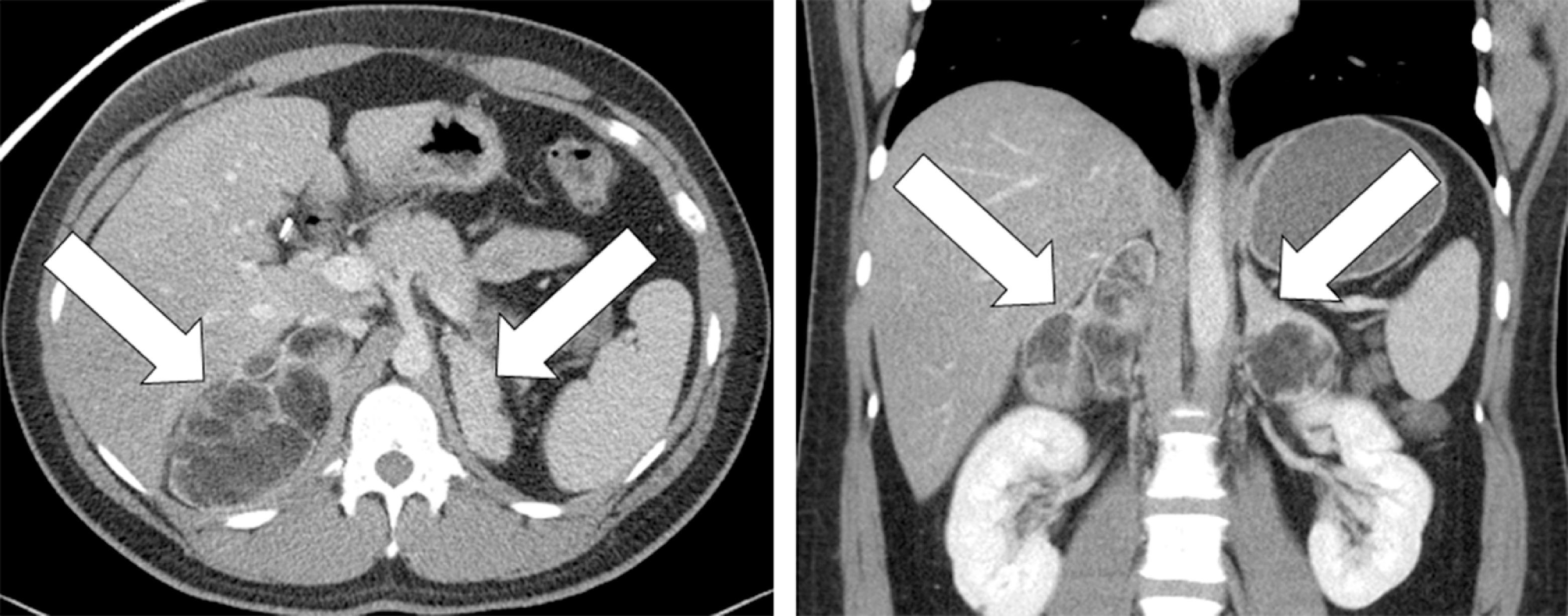
The patient was a 26-year-old man referred for evaluation of incidentally discovered bilateral adrenal masses. The patient had an episode of acute gastroenteritis that led to the CT scan ( Fig. 82.1 ). The contrast-enhanced abdominal CT scan showed multiple large bilateral adrenal macroscopic fat-containing masses and marked cortical hyperplasia, imaging findings that were diagnostic of untreated CAH. The patient recalled being treated with hydrocortisone when a young child. However, this treatment was stopped at 14 years of age. On physical examination his body mass index was 27.8 kg/m 2 and his blood pressure and heart rate were normal. The patient appeared well and was not hyperpigmented.
INVESTIGATIONS
The laboratory studies were consistent with CAH with 61-fold and 15-fold elevations above the upper limits of the reference ranges for 17-hydroxyprogesterone and androstenedione, respectively ( Table 82.1 ). Sequence analysis of CYP21A2 identified a homozygous pathogenic variant (g.655A/C>G).
| Biochemical Test | Result | Reference Range |
| Sodium, mmol/L Potassium, mmol/L Creatinine, mg/dL 17-Hydroxyprogesterone, ng/dL Androstenedione, ng/dL DHEA-S, mcg/dL Total testosterone, ng/dL Bioavailable testosterone, ng/dL ACTH, pg/mL | 137 4.2 0.9 13,400 2,250 206 736 523 445 | 135–145 3.6–5.2 0.8–1.3 <220 <150 89–457 240–950 83–257 10–60 |
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Lynch Syndrome
Adrenocortical Carcinoma Associated With Lynch Syndrome
 Metastatic Paraganglioma: Role for Systemic Chemotherapy
Metastatic Paraganglioma: Role for Systemic Chemotherapy
 Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


