##
Adrenal metastasis should be suspected in any patient with a history of extraadrenal malignancy presenting with an indeterminate adrenal mass. Full hormonal workup and assessment of imaging characteristics are important even when the likelihood of adrenal metastasis is high. , Pheochromocytoma presents with similar indeterminate adrenal imaging, and, if mistaken for an adrenal metastasis, a biopsy can be inadvertently performed, resulting in potentially severe side effects. , Imaging characteristics of the adrenal mass can help exclude malignancy (as in lipid-rich tumors), and avoid additional testing, such as adrenal biopsy. , Finally, finding adrenal hormonal excess such as cortisol, androgen, or aldosterone excess can help diagnose an adrenocortical adenoma or carcinoma and exclude other etiologies of adrenal tumors that are incapable of steroid production.
Case Report
The patient was a 66-year-old woman who was referred for evaluation of a newly found left 2.2 cm adrenal mass discovered on a contrast-enhanced computed tomography (CT) of the abdomen performed for breast cancer staging.
In addition to a recently diagnosed locally advanced left breast adenocarcinoma, the patient’s past medical history was positive for hypertension and primary hypothyroidism. Her medications included levothyroxine and hydrochlorothiazide. At the time of evaluation, she had no symptoms to suggest adrenal hormonal excess and review of systems was negative. On physical examination, her body mass index (BMI) was 27.38 kg/m 2 , blood pressure was 135/80 mmHg, and heart rate was 98 beats per minute.
INVESTIGATIONS
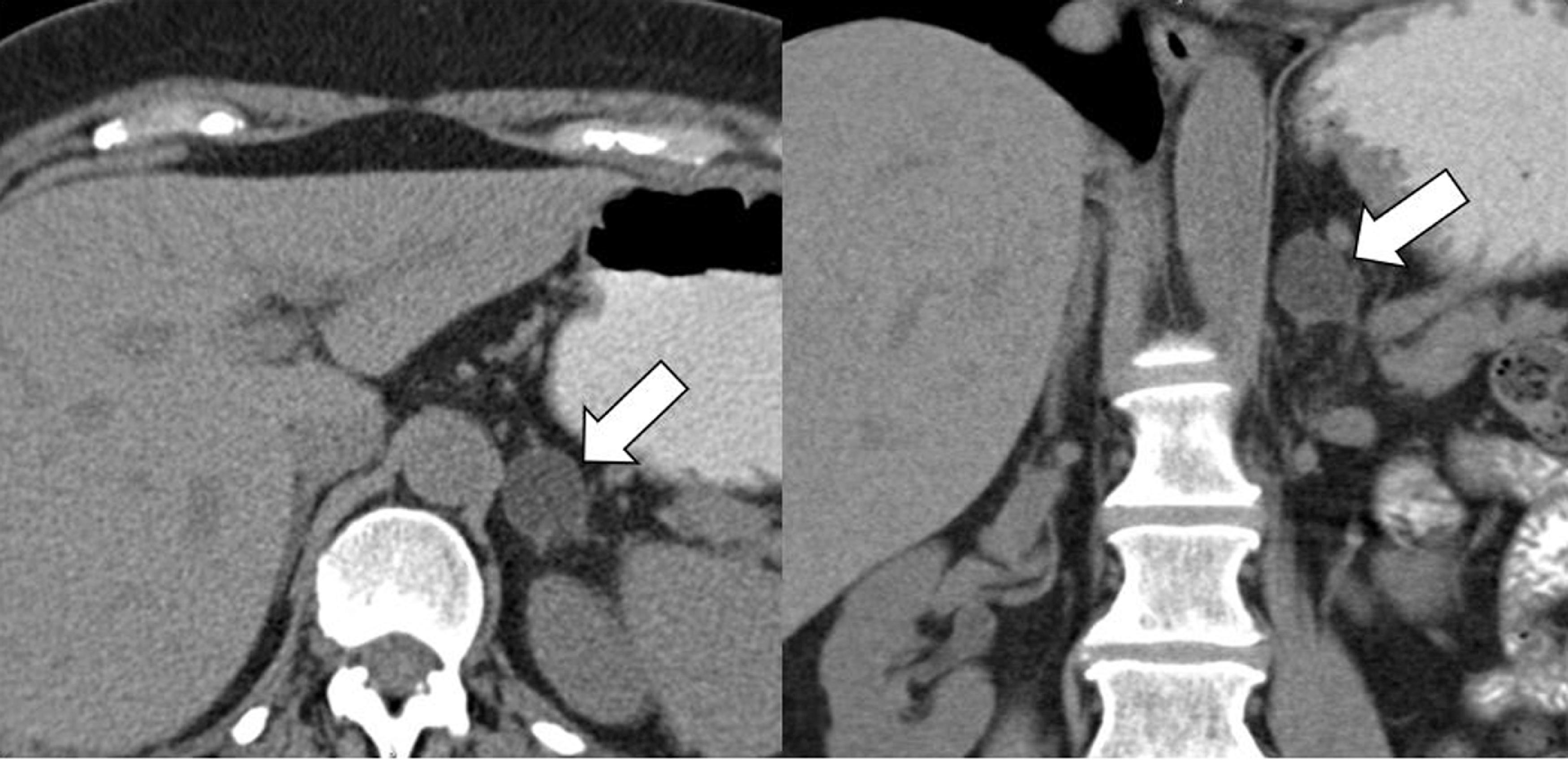
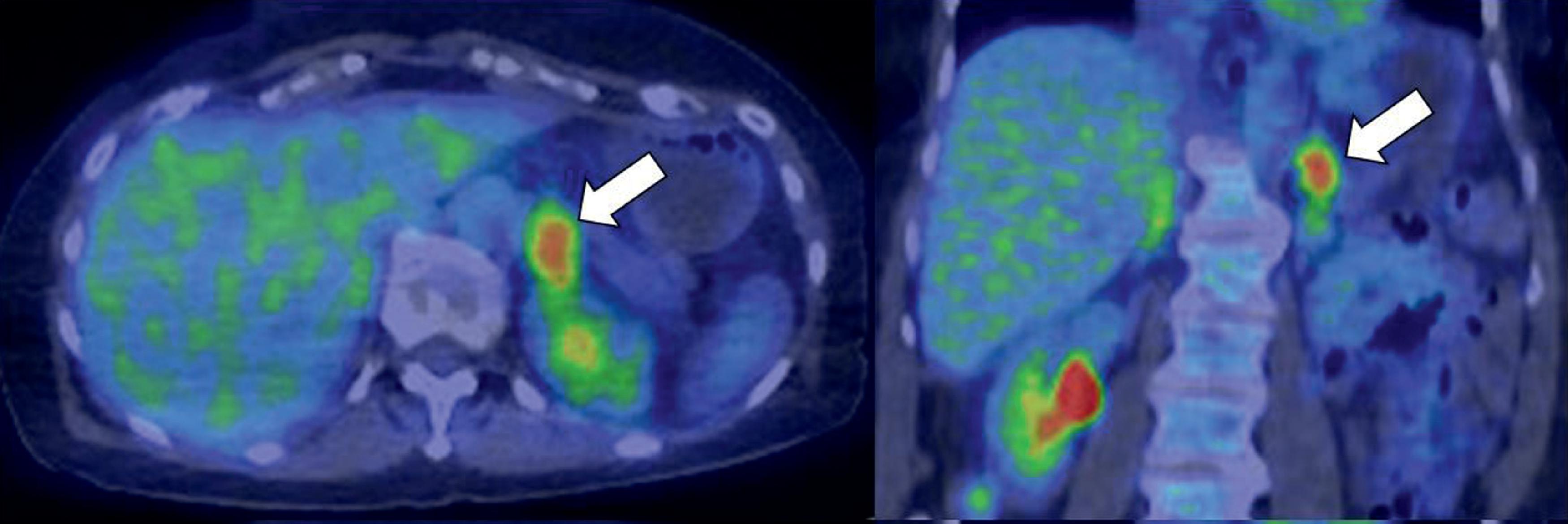
Baseline laboratory testing was obtained, and functioning pheochromocytoma and primary aldosteronism were excluded. However, the overnight dexamethasone suppression test was abnormal, and the patient was diagnosed with mild autonomous cortisol secretion (MACS) ( Table 2.1 ) . An unenhanced CT scan was obtained ( Fig. 2.1 ) and demonstrated that the 2.2 × 2.0 × 1.8 cm left adrenal mass had an attenuation of −15 Hounsfield units (HU). A F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) scan was performed at the same time for breast cancer staging and revealed that the adrenal mass had FDG uptake of 5.3 maximum standard unit value (SUVmax) ( Fig. 2.2 ).
| Biochemical Test | Baseline | 1 Year Later | 2 Years Later | 6 Years Later | Reference Range |
| Post 1-mg DST serum cortisol, mcg/dLACTH, pg/mLDHEA-S, mcg/dLAldosterone, ng/dLRenin plasma activity, ng/mL per hourPlasma metanephrine, nmol/LPlasma normetanephrine, nmol/L | 2.630348.11.30.20.63 | 3.1 | 2.554.2 | 2.92151 | <1.810–6015–157<21<0.6–3<0.5<0.9 |
Related posts:
 66-Year-Old Woman With Corticotropin-Independent Hypercortisolism and Bilateral Macronodular Adrenal Hyperplasia
66-Year-Old Woman With Corticotropin-Independent Hypercortisolism and Bilateral Macronodular Adrenal Hyperplasia
 Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
 Cryoablation Therapy for Metastatic Paraganglioma
Cryoablation Therapy for Metastatic Paraganglioma
 Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


