Indications
The indications for the abdominoinguinal incision are: (1) abdominal or pelvic tumors extending over the iliac vessels; (2) tumors in the iliac fossa; (3) primary tumors, possibly involving the iliac vessels or large iliac lymph node metastases; (4) tumors with fixation to the wall of the true pelvis or large obturator nodes; (5) tumors involving the pubic bone with or without extension to the pelvis or adductor group of muscles; and (6) tumors of the groin when they involve the vessels or the lower abdominal wall or extend in the retroperitoneal area.4,5
 Procedure
Procedure
 Position and Incision (Fig. 10.1)
Position and Incision (Fig. 10.1)
With the patient in the supine position, a lower midline abdominal incision is outlined from just above the umbilicus to the pubic symphysis. The peritoneal cavity is entered, and exploration is carried out to assess the extent of disease. Preliminary dissection between the tumor mass and visceral pelvic structures may be carried out. Involvement of the latter does not necessarily mean unresectability, of course, since they can often be removed en bloc with the tumor. When there is a question of involvement of the iliac vessels, proximal control is secured; the common iliac vessels are dissected free and vessel loops are passed around them.6
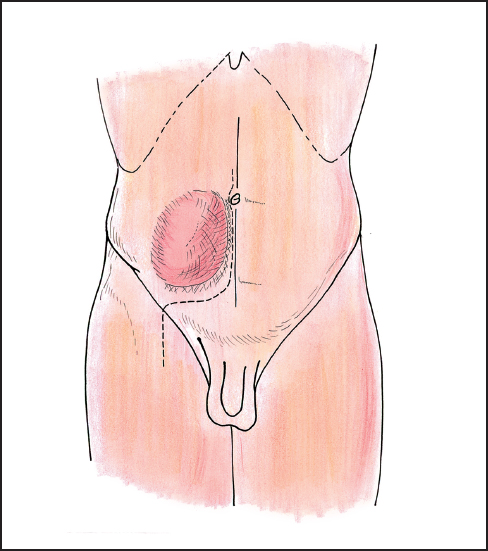
Fig 10.1 Position and incision.
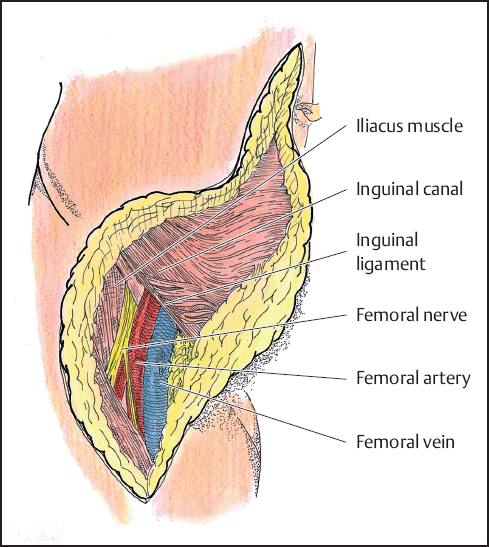
Fig 10.2 Incision through inguinal canal.
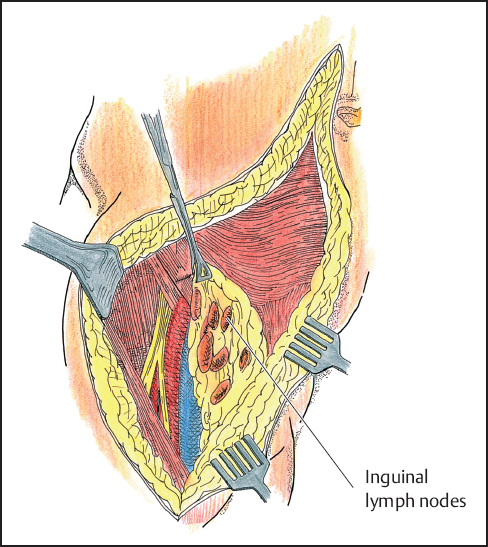
Fig 10.3 Dissection of inguinal nodes.
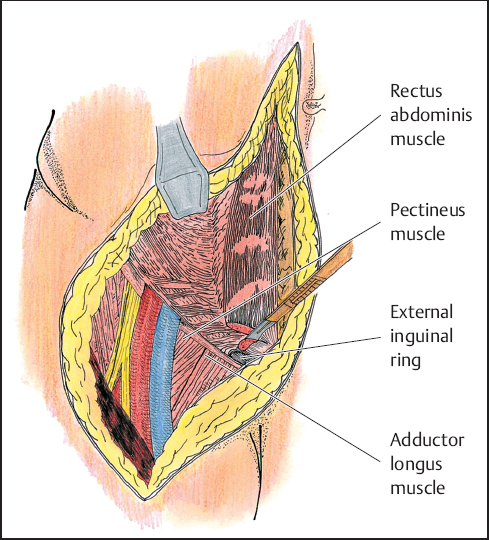
Fig 10.4 Division of rectus abdominis muscle.
 Incision through the Inguinal Canal (Fig. 10.2)
Incision through the Inguinal Canal (Fig. 10.2)
If the decision is made to proceed with the resection, the lower end of the incision is extended transversely to the midinguinal point and then vertically longitudinal to the course of the femoral vessels. The vertical portion of the incision is deepened to expose the common femoral vessels. If necessary distal control with vessel loops is second at this time.
 Dissection of the Inguinal Nodes (Fig. 10.3)
Dissection of the Inguinal Nodes (Fig. 10.3)
When the operation is performed for large iliac and/or obturator nodes or if there is clinicalor potential microscopic involvement of the inguinal nodes, the vertical portion of the incision is made to extend to the apex of the femoral triangle, flaps are raised as in a groin dissection, and the nodes are mobilized off the femoral vessels, but their proximal continuity with the deep nodes is preserved.7
 Division of the Rectus Abdominis Muscle (Fig. 10.4)
Division of the Rectus Abdominis Muscle (Fig. 10.4)
The transverse portion of the incision is deepened to the surface of the anterior rectus sheath which is divided. The rectus abdominis muscle is transected a few millimeters from its origin on the pubic crest. This incision is through its tendinous portion.
 Opening the Inguinal Canal (Fig. 10.5)
Opening the Inguinal Canal (Fig. 10.5)
The round ligament in women is divided over the pubic tubercle. In men, if the tumor is not too close to the internal inguinal ring, the spermatic cord can usually be preserved. If the spermatic cord cannot be preserved it is usually necessary to resect the testicle or it will infarct causing postoperative pain. The medial crus of the external inguinal ring is divided close to the pubic tubercle. The external oblique aponeurosis is split from the external inguinal ring lateral as in an inguinal herniorrhaphy.
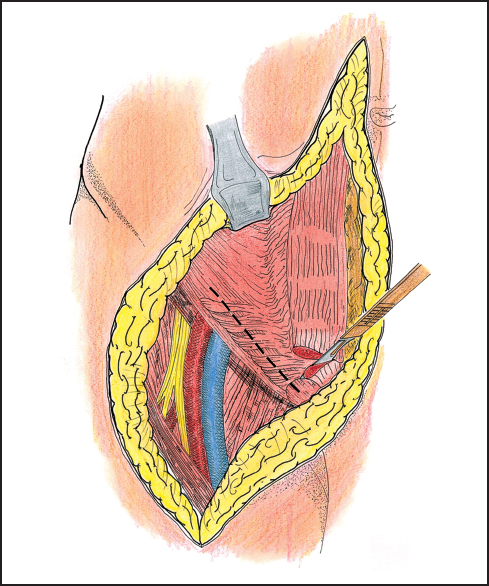
Fig 10.5 Opening the inguinal canal.
 Incising the Floor of the Inguinal Canal (Fig. 10.6)
Incising the Floor of the Inguinal Canal (Fig. 10.6)
The inguinal canal floor is divided in the same direction up to and including the medial border of the internal inguinal ring. In so doing, the spermatic cord is displaced. Alternatively, after division of the medial crus, the inguinal floor may be incised from inside and the cord exposed from within the abdomen. The testicle is extracted from the inguinal canal and scrotum for medial displacement. Deep to the internal inguinal ring the structures of the cord deviate, the vas deferens coursing medially, and the internal spermatic vessels toward a lateral and cephalad direction. Depending on the location of the tumor, the internal spermatic vessels may have to be divided at this level; if the cord structures are divided above the bifurcation of the vas deferens there is a viable ipsilateral testis. Division of the cord at the level of the external inguinal ring does not require ipsilateral orchiectomy but will be accompanied by testicular atrophy.
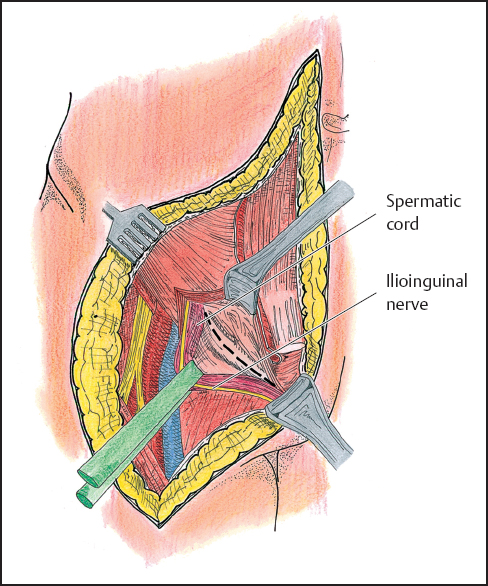
Fig 10.6 Incising the floor of the inguinal canal.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


