CLINICAL PRESENTATIONS
Part of “CHAPTER 75 – CUSHING SYNDROME“
The clinical manifestations of Cushing syndrome are determined by the increased abnormal secretion of cortisol, ACTH, and other adrenocortical steroids under ACTH control. However, the clinical presentation varies among the different types.
CORTICOTROPIN-DEPENDENT CUSHING DISEASE
Patients with pituitary ACTH-dependent disease (i.e., Cushing disease) usually have a history of disease that begins 2 to 3 years before a definitive diagnosis is made. In milder cases, symptoms may be present for 5 to 10 years. Earliest symptoms include weight gain, progressive changes in physical appearance, hypertension, and glucose intolerance. Patients may have been treated for these conditions with weight-reduction diets, antihypertensive drugs, and oral hypoglycemic agents. The
response to diet is frequently unsuccessful. Those who do not experience actual weight gain notice redistribution of adipose tissue resulting in changes in appearance, with facial rounding, increased central adiposity, and thinning of upper and lower extremities.
response to diet is frequently unsuccessful. Those who do not experience actual weight gain notice redistribution of adipose tissue resulting in changes in appearance, with facial rounding, increased central adiposity, and thinning of upper and lower extremities.
After 2 to 3 years of mild symptoms, additional symptoms or increased severity of the initial symptoms draw patients to the attention of the physician. Patients relate the appearance of striae, easy bruising, and increased body hair growth; irregular menses or amenorrhea may be present in women or gynecomastia in men. Proximal muscle weakness and atrophy are common, and some patients exhibit manifestations of a steroid myopathy. Other manifestations include peripheral edema, back pain, and loss of height if patients have developed severe osteoporosis and compression fractures of the vertebrae (Fig. 75-6A).
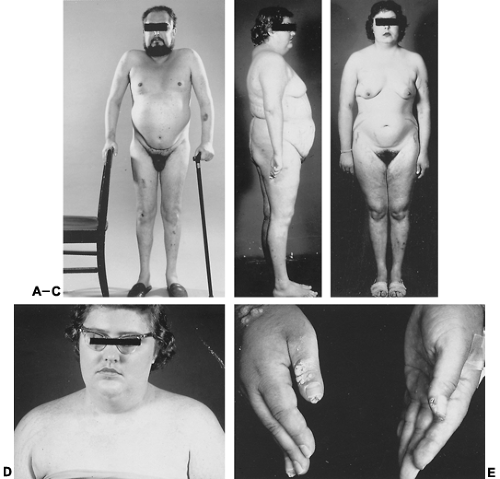 FIGURE 75-6. A, A 45-year-old man with a 2-year history of progressive muscle weakness and atrophy, truncal obesity, severe back pain, loss of height, and multiple ecchymoses. B, Truncal obesity with a very prominent cervicodorsal fat pad (i.e., buffalo hump) in a woman with Cushing syndrome. C, Atrophic striae over hips, breasts, and axillae in a 24-year-old woman with Cushing syndrome. D, A 28-year-old woman with Cushing syndrome. She had pigmented lesions of tinea versicolor over the anterior upper chest. E, Severe, intractable verruca vulgaris lesions over the fingers in a 32-year-old man with Cushing syndrome and a markedly depressed T-lymphocyte count.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|



