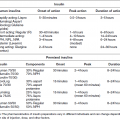
Case 4 Ira B. Lamster, DDS, MMSc; Nurit Bittner, DDS, MS; and Daniel Lorber, MD A 67-year-old male presented with the chief complaint, “My top partial denture bothers me and the teeth on my top right hurt.” The patient noticed some bleeding when brushing. He also mentioned that his mouth was feeling dry. The patient has not been to the dentist in the past three years. The patient is 5ʹ 6ʺ tall and he weighs 185 pounds. He states that he has no allergies. The patient was diagnosed with type 2 diabetes mellitus eight years ago. At that time his HbA1c was 9.5%. He was given a course of treatment consisting of lifestyle changes (exercise and diet control) and oral medications (metformin 1,000 mg bid and glimepiride 2 mg qd). He has minimal follow-up with his primary care physician and does not see an endocrinologist. With questioning, he notes paresthesia of his feet (“It feels like I am walking on clouds”) and recently fractured his wrist with minimal trauma. The orthopedist noted bone loss on his examination and recommend a test for bone density, which has not yet been performed. His last medical visit was three months ago, revealing an HbA1c of 9.1%. His primary care physician referred him to an endocrinologist; the appointment is pending. The patient does not smoke cigarettes, and denies any history of alcohol abuse. He has not used recreational drugs for the past 20 years. All of the patient’s restorations, including the porcelain fused to metal splinted crowns on the maxillary premolars and the single crowns on the maxillary first molars, were delivered more than seven years ago, in conjunction with the maxillary and mandibular removable partial dentures. The last dental visit was three years ago. At that time the patient’s current maxillary removable partial denture was repaired as tooth #9 was added to the denture when the natural tooth fractured (Figure 1). Figure 1 Maximum intercuspation, anterior view. The muscles of mastication and facial expression were all within normal limits. The temporomandibular joint was also within normal limits. The skin around the lips appeared dry and flaky. Areas of the tongue, floor of the mouth, hard and soft palate, and buccal mucosa had an erythematous appearance. A screening for oral cancer was negative. Moderate plaque and subgingival calculus deposits were observed; moderate to severe gingival inflammation was present. The mouth appeared dry, with minimal saliva. Probing depths ranged from 2 mm to 10 mm, with pronounced bleeding on probing. The maxillary right first molar and the mandibular left central incisor had grade three mobility. Furcation involvement was also noted on the maxillary right first molar. In some areas the papillae were absent, and more commonly hyperplasia and severe inflammation were noted (Figures 2 and 3). Recurrent caries were noted for many teeth. The patient claims to brush his teeth twice a day but he does not use dental floss. Figure 2 Maxillary occlusal view. Figure 3 Mandibular occlusal view. All maxillary porcelain fused to metal crowns (#3, 4, 5, 12, 13, and 14) demonstrated recurrent caries. The root tip of tooth #9 was still present, with coronal decay. Teeth #21, 28, and 32 presented with defective amalgam restorations with recurrent caries. Tooth #27 presented with a defective porcelain fused to metal crown, and recurrent caries. Pulp testing was completed for the maxillary right side because the patient complained of pain. It was determined that teeth #3 and 4 had irreversible pulpitis. Although the patient was partially edentulous and an occlusal classification could not be made, with his current removable partial denture the patient showed an Angle’s Class III occlusal scheme, which is related to the patient’s maxillo-mandibular ridge relationship. No interferences were observed on excursive movements. Full mouth series and panoramic radiographs were taken. The lamina dura was visible. Radiographic evaluation revealed minimum generalized horizontal bone loss. Teeth #9 and 13 had endodontic treatment, both demonstrating a periapical radiolucency. Teeth #3, 4, 5, 12, 13, 14, 21, 27, 28, and 31 presented with recurrent decay. The recurrent decay was more advanced on teeth #3, 4, 5, 12, 13, and 14, with both coronal and subgingival (root) involvement. The following problem list was compiled after review of the history and clinical and radiographic data: Based on the patient’s medical history of poorly controlled type 2 diabetes mellitus and the current dental findings including xerostomia, papillary hyperplasia, and denture stomatitis, it was decided to evaluate the erythematous lesion on the patient’s palate for Candida albicans infection. Infection with Candida was confirmed via culture and microscopic evaluation of a tissue swab. The patient was treated with Nystatin suspension and was instructed to soak his current removable partial dentures in the Nystatin suspension overnight as well to eliminate fungus colonization of the denture. The xerostomia was believed to be a contributory factor to the fungal infection. The patient’s metabolic control remained poor on the current drug regimen. This was changed, and the patient was placed on a combination of long-acting insulin (detemir 40 units hs) with metformin (1,000 mg bid) and sitagliptin (100 mg qd) during the day. The initial dental treatment plan consisted of reinforcement of the oral hygiene instructions, treatment for candidiasis, and palliative treatment for the xerostomia using rinses and lozenges and sipping water frequently. A full mouth scaling and root planning followed the initial patient education. Furthermore, the patient was urged to follow up with the endocrinologist because successful treatment of his dental problems depended upon achieving adequate metabolic control. Due to the advanced recurrent and root caries affecting all remaining maxillary teeth, which was in close proximity to the pulp, the prognosis for all remaining maxillary teeth was poor and extraction was recommended (#3, 4, 5, 9, 12, 13, and 14). Because the retention of the maxillary denture was a concern due to the patient’s xerostomia, the possibility of a maxillary implant retained overdenture was discussed with the patient. Restoration with implants depended on the level of metabolic control, which has proven to be a challenge. The restorative treatment plan for the mandibular arch consisted of a fixed partial denture on teeth #21– 23 and single porcelain fused to metal survey crowns on teeth #27, 28, and 31. A metal-based mandibular removable partial denture will be fabricated. Upon completion of the prosthodontic treatment the patient will be placed on a frequent recall schedule (every three to four months). A restorative follow-up will be recommended as well to monitor recurrent caries and root caries on the mandibular restorations. Due to the patient’s history and poor metabolic control, topical fluoride treatment will be part of the follow-up plan. During the next few months, metabolic management of the diabetes was improved with an HbA1c of 6.9%. Considering the improved metabolic control, after discussion with the dentist, the endocrinologist felt that the comprehensive treatment plan could begin. After the denture stomatitis was resolved (following treatment for Candida infection and improvement in metabolic control), and the initial phase of scaling and root planing, the restorative treatment began. The restorative treatment consisted first of fabrication of a maxillary immediate complete denture. All remaining maxillary teeth were extracted and the maxillary immediate complete denture was delivered with a tissue conditioner for the first week. The oral surgery was uneventful, but healing of the extraction sites was delayed. The tissue conditioner was replaced with a soft reline material that was changed periodically as deemed necessary by evaluation of the changes of the soft tissue, and to improve retention. After healing of the maxillary extractions and after the immediate denture was completely adjusted and a final reline completed, the patient continued to complain of poor denture retention and difficulty in adapting to the complete denture due to mouth dryness and persistent mucosal irritation. An assessment of salivary function revealed increased flow compared to the initial assessment, but the amount of saliva was still below normal.
The patient with diabetes mellitus and xerostomia
Medical history
Dental history and history of the current problem

Treatment plan
Treatment
Related posts:
 The influence of periodontal disease on glycemic control in diabetes
The influence of periodontal disease on glycemic control in diabetes
 Periodontal disease as a complication of diabetes mellitus
Periodontal disease as a complication of diabetes mellitus
 Management of the patient with diabetes mellitus in the dental office
Management of the patient with diabetes mellitus in the dental office
 Glycemic treatment of diabetes mellitus
Glycemic treatment of diabetes mellitus
 Classification, epidemiology, diagnosis, and risk factors of diabetes
Classification, epidemiology, diagnosis, and risk factors of diabetes
 6: Prosthodontic treatment for the newly diagnosed patient with type 2 diabetes mellitus
6: Prosthodontic treatment for the newly diagnosed patient with type 2 diabetes mellitus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


