Symptoms of overt glucocorticoid excess should prompt appropriate biochemical and imaging workup. In this case, despite imaging characteristics of myelolipoma and contralateral adrenal gland without abnormalities, ipsilateral adrenal adenoma was suspected in a patient with confirmed corticotropin (ACTH)-independent hypercortisolism.
Case Report
A 35-year-old woman was referred for the evaluation of low bone mineral density (L1-L4: z score of −2.5, left hip: z score of −2.0) discovered during workup of recurrent bilateral metatarsal fractures. Her medical history included obesity, hypertension (treated with hydrochlorothiazide and metoprolol), dyslipidemia, anxiety, and depression. She also complained of fatigue, generalized weakness, easy bruising, and nausea.
On physical examination, her blood pressure was 140/89 mmHg and body mass index was 40.55 kg/m 2 . She had no striae or proximal myopathy but did have a mild dorsocervical pad, supraclavicular pads, and mild rounding of the face.
INVESTIGATIONS
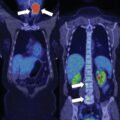
Cushing syndrome (CS) was not suspected during the initial evaluation. However, during investigation of secondary causes of osteoporosis, the 1-mg overnight dexamethasone suppression test (DST) was performed and was abnormal with a next-day serum cortisol concentration of 13 mcg/dL (normal <1.8 mcg/dL). Further testing included morning measurement of serum ACTH and dehydroepiandrosterone sulfate (DHEA-S), 8 mg overnight DST, and 24-hour urine cortisol excretion. The workup was consistent with ACTH-independent hypercortisolism ( Table 21.1 ). Unenhanced computed tomography (CT) of the abdomen was performed and demonstrated a 5.8-cm left adrenal mass with typical imaging characteristics of myelolipoma (unenhanced CT attenuation was −64 Hounsfield units [HU]) ( Fig. 21.1 ). The right adrenal gland was slightly atrophic. Despite the imaging findings pathognomonic for myelolipoma, evidence of ACTH-independent hypercortisolism and a contralateral adrenal gland without an adrenal mass led to the decision to proceed with left adrenalectomy. A collision tumor was suspected.
| Biochemical Test | Result | Reference Range |
| 1-mg overnight DST, mcg/dL | 13 | <1.8 |
| 8-mg overnight DST, mcg/dL | 12 | <1.0 |
| Morning cortisol, mcg/dL | 13 | 7–25 |
| ACTH, pg/mL | 9.2 | 7.2–63 |
| DHEA-S, mcg/dL | <15 | 18–284 |
| Aldosterone, ng/dL | 11 | <21 |
| Plasma renin activity, ng/mL per hour | <0.6 | 2.9–10.8 |
| Plasma metanephrine, nmol/L | 0.22 | <0.5 |
| Plasma normetanephrine, nmol/L | 0.7 | <0.9 |
| Urine free cortisol, mcg/24 h | 34 | 3.5–45 |
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
 Cryoablation Therapy for Metastatic Paraganglioma
Cryoablation Therapy for Metastatic Paraganglioma
 Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


