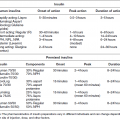
Case 3 Ira B. Lamster, DDS, MMSc; Nurit Bittner, DDS, MS; and Daniel Lorber, MD A 56-year-old woman with type 2 diabetes is being seen for a lengthy appointment for prosthodontic rehabilitation of her maxillary and mandibular arches. The patient is treated with a combination of levemir insulin (20 units hs) at bedtime and glimepiride (4 mg) in the morning. Her usual morning capillary blood glucose level is between 100 and 130 mg/dL. The only other medication she takes is levothyroxine (25 mcg qd). The patient provided a lengthy history of dental care from the time of early childhood to the present. New carious lesions occurred frequently as a child, requiring amalgam restorations in the posterior regions and composite restorations in the anterior regions. Recurrent caries and failure of existing restorations required larger restorations and single crowns. Tooth #8 was lost due to trauma and a four-unit fixed partial denture (#7–10) replaces #8. The esthetics are poor. Endodontic treatment was needed for a number of teeth, and tooth #19 was lost as a result of a failed endodontic treatment. A three-unit fixed partial denture now replaces #19. Many of the existing restorations demonstrate marginal deficiencies and recurrent caries. The patient is concerned with poor anterior esthetics. It was decided that a complete prosthodontic rehabilitation is required. Mild to moderate periodontitis is present. Periodontal surgery will be required to eliminate excessive probing depths before the final restorations are completed. An early morning appointment is scheduled to begin the crown preparations. The patient is not NPO for the procedure, eats breakfast, and takes her normal dose of insulin and oral medication. During the procedure, the patient suddenly becomes confused, diaphoretic, and tachycardic. How should this situation be managed? The treating dentist suspects dysglycemia, but is unsure if the acute physiologic reaction is due to hypoglycemia or hyperglycemia (Figures 1 and 2). In either case, immediately discontinue the procedure. If possible, check the fingerstick glucose (the patient may have a meter with her and may have a family member who can assist; Figure 3). If the glucose level is less than 70 mg/dL or if a meter is not available, treat with 4 oz fruit juice or flat regular soda (one spoonful of sugar in a glass of soda will remove the carbonation). Figure 1 Symptoms of hypoglycemia. Modified from http://www.lifeclinic.com/focus/diabetes/kids_symptoms.asp (accessed January 3, 2014). Figure 2 Symptoms of hyperglycemia. Modified from http://www.lifeclinic.com/focus/diabetes/kids_symptoms.asp (accessed January 3, 2014). Figure 3 There are more than 60 blood glucose meters on the U.S. market, and they vary in terms of cost, function, size, memory, and accuracy. The models shown are in common use at the time of this writing. Clockwise from upper left: Accu-check Nano®, Accu-check Aviva®, Bayer Contour®, One-touch Ultra Mini®, and One-touch Ultra®. Continuous glucose meters are also available, and provide a constant, real-time assessment of the blood glucose level. These devices are generally used as part of continuous subcutaneous insulin infusion, and an illustration is provided in Figure 1, in Case 1.
A patient with diabetes mellitus has a hypoglycemic episodein the dental office
Medical history
Dental history and history of the current problem
Treatment
Discussion
Related posts:
 The influence of periodontal disease on glycemic control in diabetes
The influence of periodontal disease on glycemic control in diabetes
 Periodontal disease as a complication of diabetes mellitus
Periodontal disease as a complication of diabetes mellitus
 Management of the patient with diabetes mellitus in the dental office
Management of the patient with diabetes mellitus in the dental office
 Glycemic treatment of diabetes mellitus
Glycemic treatment of diabetes mellitus
 4: The patient with diabetes mellitus and xerostomia
4: The patient with diabetes mellitus and xerostomia
 6: Prosthodontic treatment for the newly diagnosed patient with type 2 diabetes mellitus
6: Prosthodontic treatment for the newly diagnosed patient with type 2 diabetes mellitus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


