Jerome W. Conn, Professor Emeritus, University of Michigan. (From Office of the Home Secretary, National Academy of Sciences. Biographical Memoirs V.71; © 1997 The National Academies Press)
Dr. Jerome Conn belongs to the “golden age” of endocrinology, a time during the mid-twentieth century characterized by an explosion of interest in and discovery of classical endocrine hormones and the clinical syndromes produced by their dysregulation. It was a time when clinical biochemists worked side by side with inquisitive physician investigators, each one coming to the other for advice, even exchanging letters discussing the nuances and suggesting novel tests and solutions for individual patient cases. With scientific and clinical chemistry collaboration, a keen eye for clinical observation and the ability to admit patients to an investigation ward for months on end, Dr. Conn and others of his generation were able to unravel both rare and now common endocrinopathies that have since defined endocrinology practice around the world.
“Jerry” was born in New York City in 1907, the son of a lunch-shop owner. After graduating from Rutgers University in 1928, he received his M.D. from the University of Michigan in 1932 and remained at that institution for his entire career. His university expenses were paid by his two sisters who worked as secretaries to support him [1]. After a brief, 1-year flirtation with surgery, he switched to internal medicine and joined the Division of Clinical Investigation as assistant professor in 1938. At first, he worked under the supervision of Dr. Louis Newburgh who had clinical interests in the areas of diabetes and obesity. When Dr. Newburgh left to join the US Naval Research efforts, Dr. Conn became the director of the Division of Endocrinology and Metabolism in 1943, a position he held until his retirement 30 years later.
With World War II underway and the USA heavily involved in the South Pacific theatre, there was much interest in biomedical research of military importance. Dr. Conn became particularly interested in the science behind human acclimatization to heat and in 1950 published a complex paper in the Journal of Clinical Endocrinology and Metabolism demonstrating that the concentrations of sodium and chloride in human sweat were governed by steroids secreted by the adrenal cortex . In the same paper, he was able to demonstrate that the sweat electrolyte pattern could be used to evaluate the function of what he called “salt-active corticosteroids” [2]. In 1952, Simpson, Tait, and Bush isolated and identified a compound that eventually became known as “aldosterone” and thus opened the door to direct clinical measurement of Conn’s “salt-active corticosteroid.”
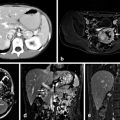
The clinical implications were not far behind these groundbreaking chemists’ work. In June and November of 1954, Dr. M. D. Milne at Hammersmith Hospital in London and Dr. C. L. Cope (also in London) published separate reports of the same patient they had shared with an apparent diagnosis of “potassium-wasting nephritis” [3, 4]. The subject, a 41-year-old Nigerian woman had presented with severe hypertension and profound hypokalemic paralysis. Milne and Cope confirmed urinary potassium wasting and a high level of urinary “electrocortin” (aldosterone) but did not appear to fully appreciate the connection and so a primary renal disease was postulated. Perhaps due to his established interest in adrenal steroids’ effect upon electrolytes, it seems that Dr. Conn had begun similar investigations on a similar patient that same year but with a clearer understanding of the likely adrenal nature of his patient’s problem. At the Central Society for Clinical Research meeting in October of 1954, Mader and Iseri from Detroit presented a paper detailing a case of hypertension and hypokalemia wherein an adrenal tumor had been found at surgical exploration in February of that year. But it was at the meeting’s presidential address that Dr. Conn presented his own index case of what he called “primary aldosteronism” . The patient was a 54-year-old woman with episodic weakness for several years. Over a 7-month inpatient investigation, Dr. Conn documented all the cardinal features of the syndrome: hypertension , hypokalemia not corrected with potassium salts, urinary potassium wasting, alkalosis, impaired urinary concentrating ability not corrected with vasopressin (hypokalemic nephrogenic diabetes insipidus). She had a low sodium to potassium ratio in her sweat and saliva, suggesting overproduction of a sodium-retaining substance. Conn postulated an aldosterone secreting adrenal tumor and indeed, an adrenal mass was discovered and surgically removed on December 10, 1954. The patient’s potassium and blood pressure normalized within 12 days with disappearance of the polyuria and muscle weakness. This presentation appeared in print in January 1955 [5] and is considered the first published description of the disease with the appropriate linkage to primary aldosterone excess. A study of the literature of the time shows that within 4 years, this new disease was being called “Conn’s syndrome” in the regular medical literature. Understanding of this newly described disease exploded and by 1962, Dr. Conn published a paper showing that his eponymous disease was not a rarity; in fact, within those 7 years, 145 similar cases were reported in the literature. Many clinicians also sought advice from Dr. Conn as he reported being aware of more than 50 other cases at the time that were as yet unpublished [6].
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


