Most endometrial cancers are cured by simple removal of the uterus. For this reason, investigators have tended to focus their attention on improving methods of identifying the minority subset of patients who are at risk for recurrence after hysterectomy alone and on the selection of effective adjuvant treatments for patients with known or suspected extrauterine disease. Over the past 30 years, many studies have attempted to define the roles of surgical staging, adjuvant radiation therapy, and adjuvant chemotherapy. However, despite years of study, many long-standing questions remain about the roles of these adjuvant treatments. Several factors have contributed to this:
Although endometrial cancer is the most common gynecologic malignancy diagnosed in developed countries, locally advanced and high-risk endometrial cancers are relatively uncommon. For example, the estimated number of uterine cancers diagnosed in the United States in 2015 is 55,000, but the estimated number of disease-related deaths is only about 10,000.1 This low rate of disease-specific mortality reflects the fact that most endometrial cancers are low-grade tumors diagnosed at an early stage.
Most of the recurrence risk resides in a small subset of patients who have multiple risk factors. When studies mix patients who have more favorable cancers with the relatively small number of higher-risk patients, the benefits of adjuvant treatments are difficult to detect (Chapter 2).
The staging and histologic classification systems have changed several times during the past 30 years. These changes complicate efforts to generalize results from early studies to current practice.
Large discrepancies exist among pathologists in the assessment of histologic risk factors and even in the diagnosis of cancer versus hyperplasia. Review of histologic material by expert gynecologic pathologists leads to significant reinterpretation of results in up to 40% of cases,2,3,4,5 making it difficult to generalize results from trials and large singleinstitutional experiences to different practice settings.
To understand and to be able to articulate the potential benefits and risks of adjuvant treatments, clinicians must navigate a complex and often flawed set of trials and retrospective studies. Because the ability to understand and explain the rationale behind treatment decisions is so critical to the effective management of endometrial cancers, a primary goal of this chapter will be to summarize available data, to suggest how those data can be applied to individual clinical situations, and to explain the sources of continued controversy.
Because the aforementioned issues tend to dominate the discourse, technical aspects of radiation therapy for endometrial cancer are often taken for granted. However, a recent survey of practice at MD Anderson Cancer Center indicated that fewer than 20% of the patients receiving external beam therapy with curative intent had stage I disease; another 20% had stage II, while the majority had stage III disease or locoregional recurrences. Although the nature of our practice undoubtedly contributes to this distribution, the past decade has seen a general decrease in the use of external beam therapy for early-stage cases and an increasing appreciation of the role of radiation therapy for locoregionally advanced cancers that may require extended radiation fields, boosts to regions of high-risk or gross disease, or combined modality treatment. As a result, endometrial cancers now represent some of our most technically challenging cases. The case studies associated with this chapter will focus on some of these more complex problems.
PRETREATMENT EVALUATION
At Initial Diagnosis
The initial treatment of most patients with newly diagnosed endometrial cancer is surgery, and the results of surgery are used to assign a FIGO stage (Table 13.1) and determine the need for additional treatment. For most patients, the yield from preoperative tomographic imaging is very low, and hence, most guidelines recommend only a chest x-ray in addition to a history and physical examination and laboratory studies. However, additional preoperative imaging studies may be helpful in some cases:
TABLE 13.1 Evolution of the FIGO Staging System for Carcinomas of the Endometrium
Distant metastases including abdominal metastases and or inguinal lymph nodes
aAfter 1988, FIGO mandated that the histologic grade of the tumor should be specified with the stage for all stages. According to the 1971-1987 staging system, only the stage I category was subdivided by grade using a system that was based strictly on the architectural pattern of the tumor. The grades were designated as “grade 1, highly differentiated; grade 2, moderately differentiated with partly solid areas; grade 3, predominantly solid or entirely undifferentiated carcinoma.” After 1988, a more detailed grading system was adopted that recognized the importance of special histologic variants and nuclear atypia (Table 13.2).
bPrior to 1988, the presence of cervical involvement was determined by fractional dilatation and curettage.
cIn 2009, tumors confined to the endometrium were grouped with other tumors that invaded <½ the myometrium, and the number of stage I subcategories was reduced from 3 to 1. Tumors that involved endocervical glands without stromal invasion were moved from the stage II to the stage I category.
dIn 1988, positive peritoneal cytology was made a criterion for inclusion in stage IIIA. In 2008, after data suggested that peritoneal cytology was a weak independent predictor of prognosis, it was removed from consideration in the FIGO system.
Patients who have high-risk histologic subtypes. Because patients who have serous carcinomas or carcinosarcomas have relatively high rates of extrauterine spread, CT or PET-CT may be indicated to rule out metastases, particularly if the patient has symptoms. Some clinicians also recommend a baseline CA-125 for patients with high-risk subtypes.
Preoperative evaluation of disease extent within the uterus. MRI can provide information about the depth of myometrial invasion that can be used to guide the extent of surgical staging. However, the accuracy of MRI is heavily dependent on the methods of image acquisition.6
TABLE 13.2 FIGO Histologic Grading System (1988-)
Grade 1
5% or less of a nonsquamous or nonmorular solid growth pattern
Grade 2
6%-50% of a nonsquamous or nonmorular solid growth pattern
Grade 3
More than 50% of a nonsquamous or nonmorular solid growth pattern
Notes on pathologic grading:
Notable nuclear atypia, inappropriate for the architectural grade, raises the grade of a grade 1 or a grade 2 tumor by 1.
In serous adenocarcinomas, clear cell adenocarcinomas, and squamous cell carcinomas, nuclear grading takes precedence.
Adenocarcinomas with squamous differentiation are graded according to the nuclear grade of the glandular component.
Patients who have gross cervical or vaginal involvement. In these cases, MRI can help to clarify the site of origin (cervix or uterus) and the extent of disease in the fundus, cervix, and vagina; this in turn helps guide the initial approach to treatment with surgery or radiation therapy (CS 13.2 and 13.3).
Genetic counseling and testing to rule out Lynch syndrome should be considered for women who are <50 years old or who have a strong family history of colorectal and uterine cancers (Chapter 1).
After Hysterectomy, Prior to Initiation of Adjuvant Therapy
Any patient who is being considered for postoperative adjuvant external beam irradiation or chemotherapy should have high-quality tomographic imaging. Such imaging serves several purposes:
To rule out extrapelvic nodes that might indicate a need for extended radiation fields. As discussed in Chapter 5, cancers involving the uterine fundus can metastasize directly to the infrarenal paraaortic nodes. For patients with high-risk endometrial cancer, it is recommended that the simulation CT extend to include the renal vessels to permit reexamination of this region, particularly if there is no recent diagnostic imaging.
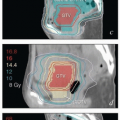
To document areas of gross disease prior to the delivery of chemotherapy for stage III disease. If the patient is subsequently referred for consolidation treatment or for disease progression, it is important to have documentation of the initial extent of disease, because more than 45 Gy is recommended to all sites of initial gross disease, even if there has been a response to chemotherapy.
To rule out suspicious nodes within the radiation therapy fields. Even modestly enlarged nodes should be considered for an integrated or sequential boost (CS 13.5 and 13.6).
To rule out distant disease. CT of the chest is recommended for most patients who have advanced-stage disease or high-risk subtypes.
Tomographic imaging should be obtained even if the patient has had an apparently complete pelvic and paraaortic lymphadenectomy. It is not unusual for residual nodes to be detected after lymphadenectomy. In our experience, the most frequent sites of residual disease after lymphadenectomy are as follows:
Posterior to and just distal to the left renal vessels
Deep to the vessels in the aortocaval space
Deep to the vessels at the point of bifurcation of the common iliac vessels (particularly on the left)
In the distal obturator region
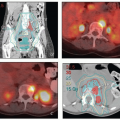
If results for preoperative imaging obtained within 6 to 8 weeks of adjuvant treatment are negative, postoperative contrast-enhanced imaging may not be needed, although all images should be carefully scrutinized by the treating radiation oncologist and compared with the postoperative treatment planning CT to confirm that all abnormal nodes have been removed. In some cases, a contrast-enhanced CT is needed to obtain good views of the nodal regions. For patients who have very extensive nodal disease, PET can be very helpful in defining radiation target volumes, although false positives due to postoperative inflammation reduce the value of PET in the immediate postoperative setting.
Before Definitive Treatment (Medically or Surgically Inoperable Cancer)
If possible, pelvic MRI should be obtained to clarify the distribution of gross disease within the uterine cavity and to assist in external beam and brachytherapy treatment planning (CS 13.2 and 13.10). For patients with high-risk histologic types, CT of the chest, abdomen, and pelvis or PET-CT should be obtained to rule out metastatic disease.
RISK ASSESSMENT
To determine the need for adjuvant therapy and to select the treatment most likely to maximize therapeutic gain, a careful assessment of risks should be undertaken to estimate:
The risk of vaginal recurrence
The risk of extravaginal pelvic recurrence
The risk of paraaortic nodal recurrence
The risk of distant recurrence
This section reviews factors that have been correlated with overall outcome and describes how these factors can be used to predict possible patterns of recurrence. Subsequent sections of this chapter address evidence that various treatments can alter these recurrence patterns and possibly contribute to cure. Ultimately, the potential gains must then be weighed against the risks of treatment-related side effects (Chapter 9).
Primary Tumor Characteristics
Several primary tumor characteristics have been commonly correlated with the outcome of patients with endometrial cancer:
Histologic subtype
Histologic grade
Presence and depth of myometrial invasion
Presence and depth of cervical stromal invasion
Lymph vascular space invasion
Tumor size
These features have all been associated with the presence of lymph node metastasis, which is in turn a strong predictor of outcome. Other extrauterine features that correlate with prognosis include vaginal, adnexal, bladder, and rectal involvement, although these are relatively rare findings. Peritoneal cytology, lower uterine segment (LUS) involvement, and cervical glandular involvement do not have a clear independent influence on outcome. Older age and African American ethnicity have been associated with poorer outcomes, although these correlations reflect, at least in part, the tendency for patients in these groups to have higherrisk tumor characteristics. Combinations of risk factors can provide much stronger predictive value than any individual feature. The current FIGO staging system (Tables 13.1 and 13.2) incorporates many but not all of the known risk factors.
Adjuvant treatment decisions are based primarily on a pathologist’s report of the operative findings. Because diagnostic errors can easily lead to inappropriate treatments, it is critical that clinicians be aware of the expertise of the pathologists interpreting their patients’ specimens (Chapter 3) and of any potential sources of error or misinterpretation. The pathologist should be consulted directly to resolve any ambiguities. Whenever possible, endometrial cancer specimens should be reviewed by a specialized gynecologic pathologist before adjuvant treatment is initiated.
The following sections discuss some of the most important predictors of outcome, with emphasis on potential sources of misdiagnosis or misinterpretation.
Histologic Variants
The five major subtypes of endometrial cancer have been categorized as type I or type II cancers according to their overall behavior:
Type I cancers tend to have a relatively favorable prognosis:
Endometrioid (75% to 80%). The differentiated features of endometrioid cancers resemble normal endometrial epithelium. Various patterns have been described, including papillary and villoglandular forms; these must not be confused with serous cancers, which also tend to have a papillary architecture but are much more aggressive. Endometrioid cancers often contain a squamous component, the grade of which typically follows that of the glandular component. Adenosquamous carcinomas are high-grade endometrioid cancers with a malignant squamous component. When low-grade cancers contain squamous elements, the squamous regions usually have a benign appearance; such cancers, which are sometimes referred to as adenoacanthomas, have a prognosis similar to that for pure adenocarcinomas of similar grade. The risk of developing endometrioid cancer is increased in patients who have been exposed to excess exogenous or endogenous estrogens, and many such cancers are to some degree hormone responsive (Chapter 1).
Mucinous (1% to 5%). The differentiated features of mucinous cancers often recapitulate cervical glandular epithelium. They typically have prominent intracytoplasmic mucin and can be difficult to differentiate from primary cervical cancers although, unlike cervical cancers, uterine cancers are usually HPV negative. Their prognosis is similar to that of endometrioid cancers.7
Type II cancers tend to be hormone independent and have a relatively aggressive behavior, even when initially confined to the uterus:
Serous (8% to 10%). The differentiated features of serous carcinomas recapitulate normal fallopian tube epithelium. Referred to in the past as “uterine papillary serous carcinoma (UPSC),” this variant is more appropriately called “uterine serous carcinoma (USC)” to accommodate cancers that have the immunohistochemical characteristics of a serous carcinoma without a distinct papillary architecture (Chapter 1).8 Virtually, all USCs are high grade, with frequent recurrence and metastasis to nodes, peritoneal cavity, and elsewhere; in this, their behavior tends to mirror that of high-grade serous cancers originating in other sites. Although USC represents only 8% to 10% of endometrial cancers, it is responsible for 40% to 50% of recurrences. Because the clinical significance of USC was not widely recognized until the mid-1980s,9,10 studies including patients treated before then should be assumed to include undetected cases of serous carcinoma. Also, because the pre-1988 grading system was strictly based on architectural appearance, USCs were often given a grade 1 or 2 assignment, further compromising the generalizability of early trials to current management. Serous carcinoma is often admixed with other subtypes. Although some authors have argued that the prognosis is somewhat better for mixed tumors than for pure serous cancers, the presence of USC tends to dominate the prognosis even when its proportion is as little as 10%.11 Underdiagnosis and overdiagnosis of serous carcinoma can lead to serious errors in treatment selection, so expert review is particularly critical.
Clear cell carcinomas (1% to 5%): Clear cell carcinoma is a rare subtype characterized by glands and papillae composed of hobnail cells having abundant clear cytoplasm. Although they have been classified as type II, clear cell carcinomas that have no serous elements are usually grade 2 and have a better prognosis than other type II cancers, with 5-year survival rates for stage I disease ranging between 75% and 95%.12 It is important to recognize that most cancers with “clear cell features” are not clear cell carcinoma. In particular, endometrioid cancers frequently have clear cytoplasm due to accumulation of glycogen, lipid, mucin, or other substances.13 Again, expert review is recommended to avoid errors in diagnosis.
Carcinosarcoma (1% to 2%): Carcinosarcomas (previously called malignant mixed müllerian tumors) are high-grade neoplasms that contain admixed malignant epithelial and mesenchymal elements. They usually occur in postmenopausal women (median age, 65) and in some cases may follow a history of pelvic radiation therapy14 or treatment with tamoxifen. Carcinosarcomas typically present as bulky, polypoid tumors that protrude through the cervical os. Deep myometrial invasion, lymph vascular space invasion (LVSI), and lymph node metastases are frequent, and pelvic and distant recurrences are common; intraperitoneal metastases are more frequent than with type I cancers, but the rate is uncertain because most authors do not distinguish between intraperitoneal and retroperitoneal abdominal metastases. In most cases, the metastases from carcinosarcomas are purely epithelial but the prognosis appears to be poorer than that for other type II cancers.
Although carcinosarcomas were previously classified as a type of uterine sarcoma or a true mixture of carcinoma and sarcoma, molecular analyses have demonstrated that most are monoclonal, with carcinomatous and sarcomatoid elements thought to represent divergent differentiation or metaplastic evolution from a common epithelial precursor.15 Carcinosarcomas are frequently subclassified as homologous (having mesenchymal elements native to the uterus) or heterologous (having foreign mesenchymal elements with features of, e.g., cartilage, bone, striated muscle, or fat), and the epithelial components can be endometrioid, serous, or clear cell. However, neither the presence of heterologous elements nor the epithelial pattern has been clearly demonstrated to be correlated with outcome.16
Histologic Grade
The current FIGO grading system is summarized in Table 13.2. Although histologic grade is one of the strongest predictors of outcome, evolving definitions and variations in the application of the current system are frequent sources of confusion:
With the 1988 system, vague definitions were made more specific and, for the first time, pathologists were advised to increase the grade if the degree of nuclear atypia was inconsistent with the architectural grade (Table 13.2). This led to a major shift in grade assignments, with a greater tendency for tumors to be diagnosed as grade 1 and with a few tumors (e.g., clear cell and serous carcinomas) assigned a higher grade than had been possible under the previous system. Because of these changes, histologic grade assignments should be viewed with skepticism for any study that included patients with tumors diagnosed before the late 1980s.
Over time, pathologists also shifted their criteria for diagnosing cancer, reclassifying some of the most welldifferentiated lesions as atypical hyperplasia.17 It is likely that many patients entered in studies prior to the mid-1980s would not be diagnosed as having cancer by current criteria; even today, the distinction between low-grade cancer and benign abnormalities can sometimes be difficult.18
Even in the modern era, studies have demonstrated major inconsistencies in the way grade is assigned.2,5 In a notable example, central pathology review of the postoperative radiation therapy in endometrial cancer (PORTEC) trials led to reassignment of ˜40% of cancers to a lower grade.19,20,21 Studies from the United States suggest a similar rate of reassignment when tumors initially diagnosed by general pathologists are subjected to expert review.2,5
Myometrial Invasion
Lymph node metastasis, recurrence, and death from endometrial cancer are all strongly correlated with the depth of myometrial invasion by tumor. Although lymph node involvement is extremely rare in patients whose cancers are confined to the endometrium, as tumor invades the underlying muscle it has access to a rich network of lymphatics that can carry metastases to the regional nodes (Chapter 5). Many methods have been used to describe the extent of myometrial infiltration. The FIGO staging system uses a threshold of 50% invasion for distinguishing stages IA and IB. Although this simple dichotomization produces two groups with different outcomes, it also diminishes the predictive power of this important variable. Strong arguments have been made for describing the degree of invasiveness in thirds,22 as a continuous variable23 or as an absolute rather than a fractional measurement.24 Although measurement of the depth of invasion is usually straightforward, significant errors can occur. Ali et al.25 reported reassignment of FIGO (1988) stage in 12% of referred cases after review by an expert pathologist. Tumors that are exophytic or involve adenomyosis can pose particular challenges. Endometrioid cancers frequently involve foci of adenomyosis that can exist deep within the uterine wall. When cancer arising in adenomyosis extends to invade adjacent myometrium, the tumor is staged according to the location of the invasive focus; however, some authors have suggested that measurement from the endomyometrial junction of the adenomyosis would more accurately predict the prognosis of such tumors.26,27
Lymph Vascular Space Invasion
LVSI has consistently been correlated with the probabilities of lymph node metastasis and locoregional recurrence23,28; these risks are increased if the LVSI is extensive.26 However, there is considerable interobserver variability in the assessment of LVSI, due in part to artifacts of processing that can mimic LVSI. Several investigators have noted that LVSI is more likely to be diagnosed and is less likely to be correlated with lymph node involvement if the uterine specimen was removed laparoscopically.29 It has been hypothesized that the balloon tip intrauterine manipulators used during laparoscopic hysterectomy can displace tumor cells into vascular spaces, causing so-called “vascular pseudoinvasion.” In some cases, this may be indistinguishable from true LVSI. More study will be needed to determine how this potential source of error should influence the use of LVSI as a prognostic factor in endometrial cancers.
Tumor Size
Several authors have found significant correlations between the diameter of the primary tumor (≤2 cm vs. >2 cm) and the presence of lymph node metastasis23,30; the tumor diameter has been variously defined as the average30 or the maximum diameter as measured on fresh tissue.23 The significance of tumor size seems to be independent of invasion depth or tumor grade.
Cervical Involvement
The presence of cervical involvement has classically been considered to be an independent risk factor for recurrence, although robust evidence supporting this can be difficult to find. Most studies of stage II disease have included patients who were classified using the inaccurate pre-1988 clinical staging system (Table 13.1) or who had FIGO 1988 stage IIA disease. Also, nearly all studies are confounded by treatment selection bias. That said, several investigators have cited cervical stromal involvement as an independent predictor of lymph node involvement.23,31 Investigators from the Mayo Clinic also reported that cervical stromal involvement was associated with poorer overall survival for patients with grade 3 or type II carcinomas but that it was not correlated with survival of patients with lower-grade cancers.32 It seems likely that the depth of cervical stromal invasion is important; however, the only studies that have examined this are small and confounded by treatment selection bias.33,34 It should be recognized that the indistinct junction between the LUS and endocervix can be a cause of significant intraobserver variability in the designation of cervical stromal involvement. Early stromal involvement can also be difficult to distinguish from involvement of invaginating endocervical glands.35
LUS Involvement
The most notable feature of tumors originating in the LUS is the high incidence (about 30%) of associated Lynch syndrome.36 Although tumors arising in the LUS are, due to their proximity to the cervix, more likely to be stage II disease, they do not seem to have an increased incidence of lymph node involvement. On the other hand, fundal carcinomas that extend to involve the LUS are likely to be large tumors with other high-risk features associated with advanced disease. The mixture of these two presentations has led to inconsistent conclusions about the prognostic significance of LUS involvement. There is, however, little evidence that LUS involvement per se is an independent predictor of prognosis when tumor size, depth of invasion, and other risk factors are taken into account.
Lymph Node Involvement and Its Influence on Prognosis
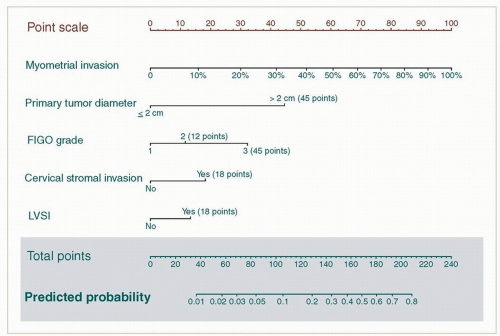
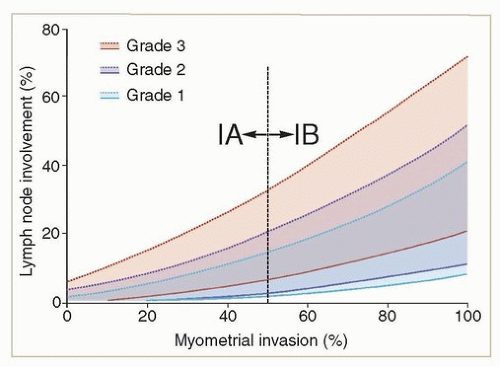
All of the adverse risk factors discussed above have been associated with an increased rate of lymph node metastases and most are independent predictors of metastasis. In 2013, AlHilli et al.23 proposed a nomogram for predicting the likelihood of lymphatic dissemination. This tool, based on findings in 883 patients from the Mayo Clinic who had lymphadenectomy or who were observed without adjuvant treatment (Fig. 13.1), demonstrates the complex relationship between intrauterine risk factors and lymph node metastasis. A reconfiguration of the Mayo Clinic data (Fig. 13.2) clearly illustrates why a simple combination of grade and depth of invasion is insufficient to predict the risk of metastasis. Although the quantitative accuracy of the Mayo Clinic nomogram needs to be validated with another dataset, it is one of the more useful tools currently available for predicting the relative risk of lymph node involvement and the need for adjuvant treatment, particularly for patients who have not had lymphadenectomy.
As discussed in Chapter 5, cancers involving the uterine fundus can spread directly to the paraaortic lymph nodes, in some cases even without evidence of pelvic node metastasis. In a prospective study of intermediate- to high-risk local features, Mariani et al.37 reported that, of 57 patients who had formal pelvic and paraaortic lymphadenectomy, 51% had involvement of both the pelvic and paraaortic nodes, 33% had pelvic node involvement only, and 16% had only paraaortic node involvement. Of 26 patients who had detailed information about the location of paraaortic nodes, 77% had metastases superior to the inferior mesenteric artery. This pattern of nodal dissemination is very different from that of cervical cancer and has important implications for radiation therapy planning.
Lymph node involvement is undoubtedly a predictor of poorer prognosis. However, several factors may influence the survival rates reported in clinical series:
Adjuvant external beam therapy reduces the rate of regional recurrence and, as will be discussed later, adjuvant treatment probably improves survival.
Variations in the extent of surgical evaluation and in the methods of histologic processing of lymph nodes are sources of significant stage migration in patients with endometrial cancer. In particular, recent interest in lymphatic mapping with sentinel node evaluation is likely to increase the proportion of patients found to have very early micrometastases or isolated tumor cells in sentinel nodes38; this may lead to an appearance of improved survival rates for patients with stage IIIC disease.
FIGURE 13.1 Mayo Clinic nomogram for the prediction of lymph node metastases, as proposed by AlHilli et al.23 The study was based on 883 patients with type I cancers who had pelvic and paraaortic lymph node dissection or who were followed without adjuvant treatment. (LVSI, lymph vascular space invasion.)
FIGURE 13.2 In this figure, the predicted lymph node rates specified in the Mayo Clinic nomogram shown in Figure 13.123 have been reconfigured to illustrate why the risks of node involvement cannot be accurately predicted using grade and depth of invasion alone. The lower (solid) lines of each color represent the predicted rate of lymph node metastases for patients with grade 1, 2, or 3 disease who have tumors <2 cm without lymph vascular space invasion (LVSI). The upper (dotted) lines represent the predicted rates for each grade if patients have larger tumors with LVSI. Note the marked overlap in risk depending on the presence or absence of risk factors other than grade and depth of invasion.
Evidence suggests that with appropriate volume-directed treatment, the prognosis of stage IIIC2 disease is not markedly different from that of stage IIIC1 tumors of similar grade.39 The influence of other nodal factors including the number of nodes, nodal ratio, and presence of gross disease has been studied to a very limited degree, with various conclusions.39,40,41,42
Other Factors
Peritoneal Cytology
Although peritoneal cytology was for many years included as a criterion for FIGO staging (Table 13.1), most evidence suggests that it is not a useful independent predictor of prognosis. For this reason, it was removed from the FIGO staging of endometrial cancer in 2009. Peritoneal cytology may have served as a surrogate for undetected serous cancers in early reviews. However, serous cancers tend to recur intraperitoneally despite negative cytology results, and endometrioid cancers rarely recur intraperitoneally even in the context of positive washings. The excellent outcome of patients who have positive results for peritoneal cytology without other risk factors suggests that the development of intraperitoneal metastasis has more to do with cancer biology than with the presence of free-floating intraperitoneal tumor cells. Some authors have reported an increased incidence of tumor cells in the peritoneal cytology of patients undergoing laparoscopic (as opposed to open abdominal) hysterectomy for low-grade cancers43; although there is no evidence that this alters prognosis, some clinicians have advocated tying the fallopian tubes to prevent tumor egress during uterine manipulation.
Molecular Markers
Investigators are currently studying a host of molecular markers that promise to refine our predictive capabilities, although none are in routine use today. See Chapter 1 for discussion of this topic.
Patient Factors
Most authors have found a correlation between increasing age and poor prognosis. This reflects, in part, the fact that older patients are more likely to have serous and other high-grade tumor types, whereas young women with endometrial cancer tend to have low-grade endometrioid cancers. However, age is often reported to be an independent predictor of prognosis even after adjustment for other known prognostic factors.32 For this reason, age is included in several definitions of “high intermediate-risk” stage I disease.19,22 Other patient factors that may be correlated with the rate of relapse are race, obesity, and diabetes mellitus.44 Overall survival is also heavily influenced by the comorbid illnesses that are often present in this group of patients32; intercurrent death is another factor that can reduce the influence of adjuvant treatments.
FIGO Stage
The FIGO staging system was converted from a clinical to a pathologic staging system in 1988 and was further modified in the most recent (2009) version (Tables 13.1 and 13.2). The current system incorporates some of the most important predictors of prognosis and is correlated with outcome, although there are few large series that have prospectively employed the 2009 version. The FIGO system is unusual for staging systems in that it requires an assessment of tumor grade and specifies criteria for assigning grade. However, as discussed above, the outcomes and proportions of patients falling into various subgroups are dependent on the experience of pathologists assigning grade, the rigor of surgical staging, and possibly on the methods of adjuvant treatment used to treat high-risk disease.
Mechanisms and Risk Factors for Vaginal Recurrence
An understanding of the mechanism of vaginal recurrences has important implications for the development of an effective preventive strategy. Dissemination through the vaginal lymphatics has been suggested as a potential route for vaginal metastasis leading to recurrence. However, several features of vaginal recurrence suggest that posthysterectomy implantation of tumor cells in surgically disturbed vaginal tissues, possibly encouraged by growth factors produced by the healing process (Chapter 3), may provide a more likely explanation.
Only gold members can continue reading. Log In or Register to continue