Typical Carcinoid Tumor
Mary Beth Beasley
Carcinoid tumors as a whole make up approximately 1% to 2% of all pulmonary malignancies and consist of typical and atypical subtypes. Atypical carcinoid tumor (AC) is discussed in detail in Chapter 11. Typical carcinoid tumor (TC) is defined in the 2004 World Health Organization (WHO) classification of lung tumors as a carcinoid tumor with fewer than 2 mitoses per 10 HPF and lacking necrosis.1 By definition, TC is >5 mm in size, which is currently the only feature discriminating TC from carcinoid tumorlet (Fig. 10-1). While a definitive precursor lesion has not been consistently identified, at least some cases, particularly peripheral TCs, appear to arise in a background of diffuse idiopathic pulmonary neuroendocrine cell hyperplasia, which is discussed in chapter 28.2,3 and 4
TC classically presents as a central endobronchial mass, although approximately a third of TC are peripheral and may not have an obvious associated airway.1,5 TCs tend to occur with a slightly higher frequency in the right lung. Central tumors in particular may be associated with stridor or obstructive symptoms, while peripheral tumors may be asymptomatic. TC occurs in a younger population than conventional lung cancers and has an average age of presentation of 45 years. Fewer than half of patients with TC are current or former cigarette smokers, and while many studies indicate approximately equal gender incidence, some studies indicate that the disease occurs slightly more frequently in women. Carcinoid syndrome is uncommon and generally occurs in the presence of liver metastases. Cushing syndrome may also be encountered and rare cases may be associated with acromegaly.1,6,7,8,9 and 10
Radiographically, features characteristic of TCs are the presence of a well-defined tumor associated with an airway, occasionally associated with punctuate or diffuse calcification. Evaluation of TCs with positron emission tomography (PET) has yielded variable results, with most studies indicating that PET has low sensitivity for detecting carcinoid tumors. TCs generally have low metabolic activity and most studies indicate that PET results often demonstrate only low or equivocal uptake.11 Octreotide scanning (somatostatin receptor scintigraphy) plays a role in imaging of carcinoid tumors due to the presence of somatostatin receptors on the tumor cells, and at least one study has reported a sensitivity of 90% and specificity of 83%.8,10
TC is generally associated with a favorable prognosis, with a 5-year survival rate of 85% to 90%, although patients with widely metastatic disease generally have a poor prognosis (14%-25% reported 5-year survival rate).8,10 The presence of lymph node metastases also impacts prognosis, although some studies have found that the prognosis is generally still highly favorable or in keeping with that of tumors without nodal metastases.12 The true incidence of nodal disease has been difficult to assess from the literature due to variable classification practices, although a number of 15% is frequently cited. A 2009 study by Wurtz et al.,13 evaluating the presence of lymph node metastases in resected TC and AC using current WHO criteria, found nodal disease in 14.3% of TC cases (N = 42). A study by Ferolla et al.14 also reported a 14% incidence of lymph node metastases in 100 TCs. In the Wurtz series, 4.8% of these cases were classified as N1 and 9.5% as N2. Interestingly, four of the N2 cases had so-called skip metastases without identification of metastatic disease in N1 nodes. All of the TCs with nodal metastases in that study were centrally located. Nodal metastases were seen more frequently in patients under age 35 and in tumors
larger than 3 cm, although N2 disease was observed in one case with a 0.7-cm tumor.13 These findings, in combination with other studies, stress the importance of lymph node dissection in TC. Treatment of carcinoid is generally surgical, most frequently lobectomy or pneumonectomy, although lung sparing procedures have been used with success.7,15,16 Chemotherapy and radiation therapy have generally been of limited value.7,10,17 Several potential therapeutic targets have been identified that are discussed in the molecular section below.
larger than 3 cm, although N2 disease was observed in one case with a 0.7-cm tumor.13 These findings, in combination with other studies, stress the importance of lymph node dissection in TC. Treatment of carcinoid is generally surgical, most frequently lobectomy or pneumonectomy, although lung sparing procedures have been used with success.7,15,16 Chemotherapy and radiation therapy have generally been of limited value.7,10,17 Several potential therapeutic targets have been identified that are discussed in the molecular section below.
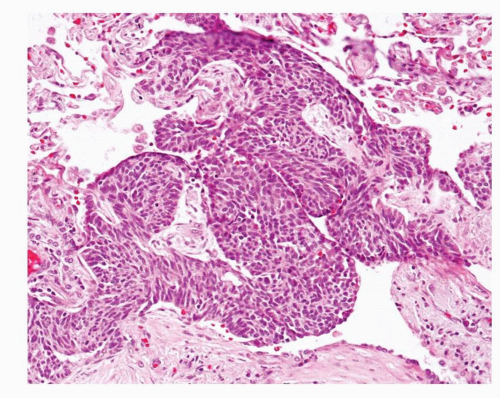 FIGURE 10-1 Medium power image of an approximately 3-mm carcinoid tumorlet. The histologic and immunohistochemical features of a carcinoid tumorlet are similar to those of a TC; however, the carcinoid tumorlet measures 5 mm in size. |
Another issue in regard to outcome that has recently been investigated in several studies is the issue of multiple carcinoid tumors and/or tumorlets and whether there is an impact on prognosis. Peripheral carcinoid tumors in particular may be associated with multiple tumorlets or multiple carcinoid tumors.18 Several studies have evaluated this issue and all have concluded that behavior is governed by the dominant carcinoid tumor and that the presence of additional carcinoid tumors does not impact prognosis.3,19 A study by Ferolla et al.,14 which identified multicentric carcinoid tumorlets in 12/100 TCs and 3/23 ACs, reported a negative impact on survival in univariate analysis; however, the significance in multivariate analysis is not stated in the paper.
Carcinoid tumors were not technically included in the 6th edition AJCC TNM Staging System of lung carcinomas, although in practice this staging system was generally applied to these tumors. Carcinoid tumors are included in the AJCC 7th Additional TNM Staging System and should therefore be staged according to the same guidelines as other lung carcinomas.20
TYPICAL CARCINOID TUMOR, CYTOLOGY
Cytologically, TCs show a monotonous population of small cells with round, uniform nuclei and abundant cytoplasm (Fig. 10-2). Hyperchromasia, increased mitotic figures, and necrosis are not characteristic of TCs; however, in some cases, nuclear atypia may be present. In some TCs, cells may exhibit a plasmacytoid appearance.
TYPICAL CARCINOID TUMOR, GROSS FEATURES
TCs are typically central but may be peripheral. They generally measure between 2 and 4 cm in diameter and are tan to yellow-red on cut section. The tumor may protrude into the airway and occasionally may obstruct the airway lumen. Hemorrhage and necrosis are not characteristic gross features of TCs ( Figs. 10-3,10-4 and 10-5).
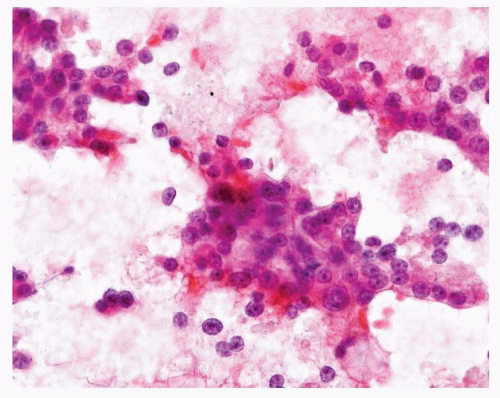 FIGURE 10-2 High-power image of Pap-stained cytology preparation of TC showing cells with round, uniform nuclei and small nucleoli, as well as conspicuous cytoplasm. |
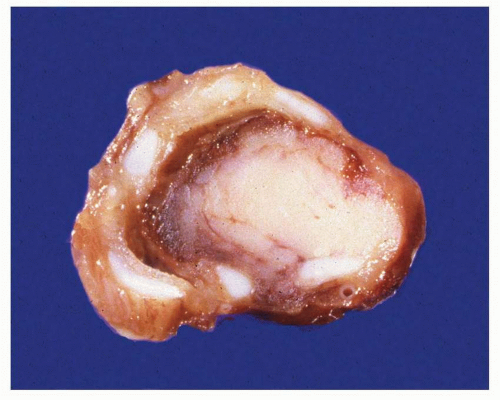 FIGURE 10-3 Gross cut section image of a central carcinoid tumor showing off-white to tan tumor, with no areas of necrosis or hemorrhage, occluding the bronchial airway. |
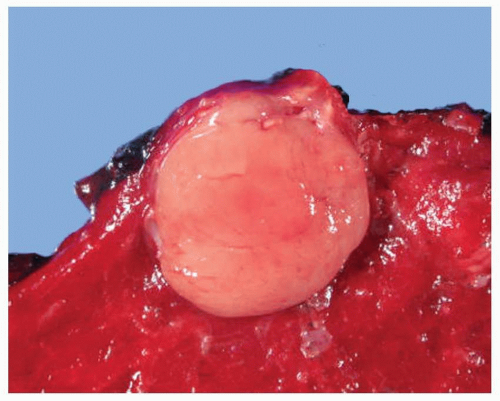 FIGURE 10-4 Gross image of a peripheral carcinoid tumor showing a wellcircumscribed subpleural off-white tumor nodule that bulges on cut section, with no areas of hemorrhage or necrosis present. |
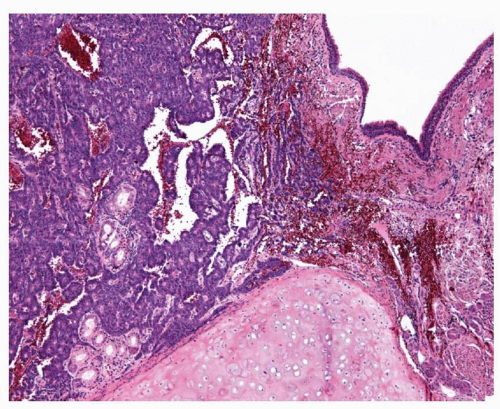 FIGURE 10-5 Low-power image of bronchial carcinoid tumor showing tumor bulging into the airway and abutting bronchial cartilage, with no necrosis present. |
TYPICAL CARCINOID TUMOR, HISTOLOGY
TC is classically composed of a uniform population of polygonal cells with central nuclei with granular nuclear chromatin and moderately abundant associated eosinophilic cytoplasm. Nucleoli are generally absent but may be encountered in some cases. The cells are generally fairly uniform in appearance; however, nuclear atypia may be present and is not a criterion for diagnosing the lesion as an AC tumor (Fig. 10-6). Organoid (Fig. 10-7) and trabecular growth patterns (Fig. 10-8) are most frequently encountered and the background stroma is highly vascular. Other patterns that may be encountered are papillary growth, a pseudoglandular pattern (Fig. 10-9), and a follicular pattern (Fig. 10-10) in which the cells are arranged around eosinophilic material resembling colloid and prominent rosette formation (Fig. 10-11).1,6 Variance in the cellular morphology may also occur and includes tumors with clear cells,21 abundant oncocytic cytoplasm, acinic cell morphology, and tumors with intracytoplasmic melanin.22,23 The stroma may similarly show unusual features such as calcification, ossification, or deposition of amyloid-like material (Fig. 10-12). Spindle cell morphology may be seen in peripheral tumors in particular (Fig. 10-13).1,6
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


