Metastatic Tumors to the Lung
Timothy Craig Allen
Metastatic tumors to the lungs are the most common lung neoplasm, and the lungs are the recipient of more metastatic neoplasms than any other organ.1,2,3 and 4 Cancers from essentially any site in the body can metastasize to the lung.5,6 and 7 The lungs are the only organ for which the entire blood and lymphatic supply flow, and their dense capillary network is often the first encountered by circulating tumor cells entering the venous blood supply from the ductus lymphaticus.1,8 The lungs are the site of metastases in 20% to 54% of cases in patients with extrapulmonary primary malignant neoplasms, and in 15% to 25%, the lung is the only site of metastasis.3,9,10 and 11 Common sites of metastatic tumors to the lung include lung, gastrointestinal tract, breast, pancreas, kidney, melanoma, thyroid, liver, and prostate.1,2 and 3,6,12,13 Lymphatic spread of tumor is commonly found with metastases from the stomach, breast, ovary, prostate, and lung; and hematogenous spread of tumor is often identified with metastases from the breast, kidney, colon, and testes.2 According to the International Registry of Lung Metastases, 44% of metastases are carcinomas, 42% sarcomas, 7% germ cell tumors, and 6% melanomas. Colorectal carcinoma comprised 33% of metastatic tumors to the lung, with 20% breast, 19% renal, 12% head and neck, 7% uterus, and 3% lung.14,15 and 16 In many cases there is a clinical history of an extrapulmonary primary tumor, and situations involving nonpulmonary occult primary tumors are relatively uncommon; however, 3% to 7% of patients with lung cancer also have another, independent, nonpulmonary primary tumor.3,14,17 In many cases, histology alone is enough to reliably diagnose the primary tumor, especially in cases where the primary is known.3,18 The major problem in diagnosing a metastatic tumor to the lung occurs in the setting of a solitary nodule, an atypical presentation such as a cavitating tumor or a central tumor, or a poorly differentiated tumor with ambiguous histological and immunohistochemical features. In some cases, it is impossible to distinguish whether a lung tumor is primary or metastatic.1,3,6,7,13,14,18,19 and 20
Clinically, patients with metastases to the lungs often do not exhibit pulmonary symptoms; however, patients with endobronchial tumor may have cough and hemoptysis as well as obstructive symptoms such as dyspnea and wheezing. Chest pain may be present if there is pleural involvement with tumor.1,3,6,13,21 Radiologically, chest x-ray, high-resolution CT scan, and PET imaging are often employed in the evaluation of patients with suspected lung metastases.1,3,22,23 While CT scan has generally replaced chest x-ray alone for the preoperative evaluation of patients with suspected metastases to the lung, PET scans and, more recently, PET/CT imaging are more frequently being used in addition to CT scan for evaluation of these patients, with results reportedly superior to CT scan alone.22,24 Along with the clinical and radiologic correlative findings, the gross and microscopic features assist in determining which, if any, immunostains or group immunostains may be valuable in further differentiating the tumor metastatic to the lung.
METASTATIC TUMORS TO THE LUNG, GROSS FEATURES
Grossly, metastatic neoplasms metastatic to the lungs typically involve the lower lobes bilaterally with multiple, often peripheral, well-circumscribed tumor nodules that range from many small military tumor nodules to large “cannonball” masses that may be confluent (Figs. 17-1 and 17-2). Solitary pulmonary nodules may also be a manifestation of metastatic disease to the lungs and
occur in 3% to 9% of cases of metastatic tumor to the lung (Fig. 17-3).1,3,6,13,23,25,26 The specific gross presentation varies with the type of metastasis; however, melanomas, germ cell tumors, and ovarian carcinomas often present with a miliary pattern, and renal cell carcinomas and sarcomas usually present with a “cannonball” pattern of metastasis. Tumor involving the lung and having a thick, rind-like layer of tumor over the lung surface may represent pleural diffuse malignant mesothelioma, metastatic tumor to the pleura with lung involvement, or primary pulmonary pseudomesotheliomatous carcinoma (Fig. 17-4). Mucin-producing adenocarcinoma metastases, such as ovarian, breast, or gastrointestinal tract metastases, may show a yellow-tan glistening mucoid cut surface, with or without areas of necrosis or hemorrhage (Fig. 17-5). A similar glistening mucoid cut surface may be seen with myxoid sarcomas, often arising primarily in the retroperitoneum or the extremities. Renal cell carcinomas, liposarcomas, adrenal cortical tumors, and sex cord stromal tumors that are metastatic to the lung often show a yellow or golden appearance, indicative of glycogen or lipid, on cut surface. Tumors that appear red or red-brown on cut section may contain diffuse hemorrhage or areas of hemorrhagic necrosis, suggestive of angiosarcoma, gastrointestinal stromal tumor, or choriocarcinoma, among others. Metastatic sarcomas and metastatic lymphomas may present a gray, “fish-flesh” appearance on cut section. Metastatic melanomas may show variable areas of black coloration (Fig. 17-6). A hard, bony or firm gritty consistency identified on cut section suggests bone- or cartilage-producing tumors such as chondrosarcoma and osteosarcoma. Other tumors that may exhibit a gritty consistency on cut section include teratoma, carcinosarcoma, and psammoma body-producing tumors such as papillary thyroid carcinoma and ovarian carcinoma (Fig. 17-7).1,2,3 and 4,6,12,13,23,25,27,28
occur in 3% to 9% of cases of metastatic tumor to the lung (Fig. 17-3).1,3,6,13,23,25,26 The specific gross presentation varies with the type of metastasis; however, melanomas, germ cell tumors, and ovarian carcinomas often present with a miliary pattern, and renal cell carcinomas and sarcomas usually present with a “cannonball” pattern of metastasis. Tumor involving the lung and having a thick, rind-like layer of tumor over the lung surface may represent pleural diffuse malignant mesothelioma, metastatic tumor to the pleura with lung involvement, or primary pulmonary pseudomesotheliomatous carcinoma (Fig. 17-4). Mucin-producing adenocarcinoma metastases, such as ovarian, breast, or gastrointestinal tract metastases, may show a yellow-tan glistening mucoid cut surface, with or without areas of necrosis or hemorrhage (Fig. 17-5). A similar glistening mucoid cut surface may be seen with myxoid sarcomas, often arising primarily in the retroperitoneum or the extremities. Renal cell carcinomas, liposarcomas, adrenal cortical tumors, and sex cord stromal tumors that are metastatic to the lung often show a yellow or golden appearance, indicative of glycogen or lipid, on cut surface. Tumors that appear red or red-brown on cut section may contain diffuse hemorrhage or areas of hemorrhagic necrosis, suggestive of angiosarcoma, gastrointestinal stromal tumor, or choriocarcinoma, among others. Metastatic sarcomas and metastatic lymphomas may present a gray, “fish-flesh” appearance on cut section. Metastatic melanomas may show variable areas of black coloration (Fig. 17-6). A hard, bony or firm gritty consistency identified on cut section suggests bone- or cartilage-producing tumors such as chondrosarcoma and osteosarcoma. Other tumors that may exhibit a gritty consistency on cut section include teratoma, carcinosarcoma, and psammoma body-producing tumors such as papillary thyroid carcinoma and ovarian carcinoma (Fig. 17-7).1,2,3 and 4,6,12,13,23,25,27,28
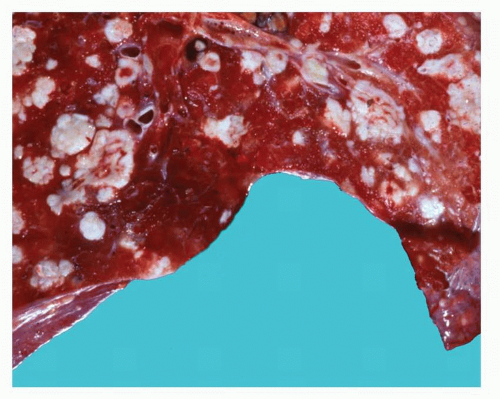 FIGURE 17-1 Gross image of lung containing numerous “cannonball” metastatic tumor nodules in a patient with a history of renal cell carcinoma. |
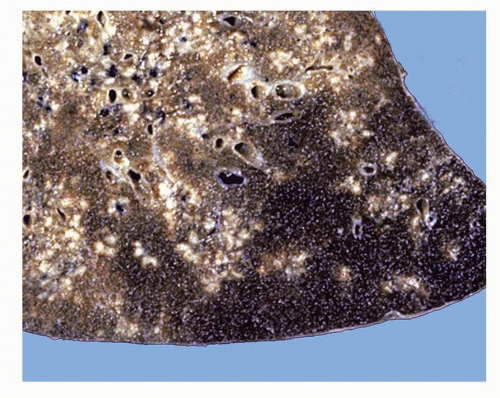 FIGURE 17-2 Gross image of lung containing numerous small tumor nodules in a miliary distribution in a patient with a history of ovarian carcinoma. |
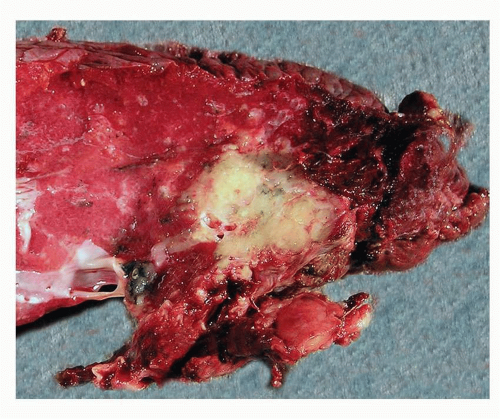 FIGURE 17-3 Gross image of lung containing a somewhat multinodular firm off-white to tan irregularly marginated tumor mass in a patient with a history of breast carcinoma. The gross image is also consistent with a lung primary neoplasm. |
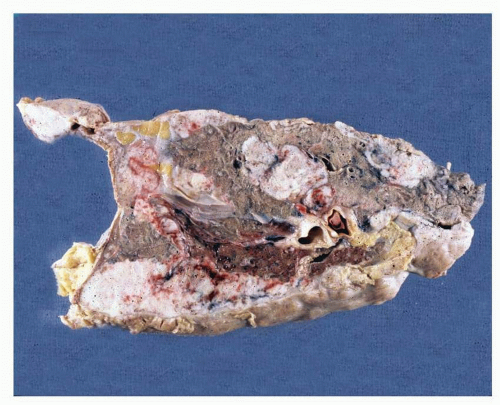 FIGURE 17-4 Gross image of “pseudomesotheliomatous carcinoma” in a patient with a history of colon carcinoma. The gross presentation is consistent with metastatic tumor to the pleura with invasion of the lung, with primary pulmonary pseudomesotheliomatous carcinoma arising in the lung and spreading in a rind-like manner along the pleura, and with pleural diffuse malignant mesothelioma arising in the pleura and spreading into the lung parenchyma. As histologic patterns may vary, clinical and radiologic correlations are very important in determining an appropriate immunostaining panel to assist in accurate diagnosis. |
 FIGURE 17-5 Gross image of lung containing a tumor mass with a glistening, mucoid cut surface in a patient with a history of mucinous ovarian adenocarcinoma. |
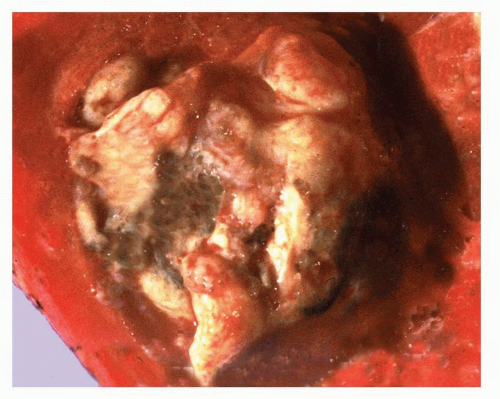 FIGURE 17-6 Gross image of lung containing a tumor mass with areas of dark brown to black coloration in a patient with a history of melanoma. |
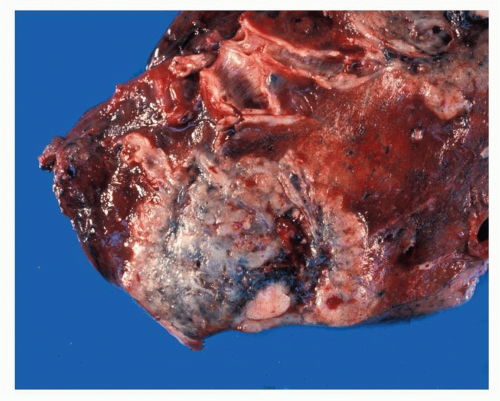 FIGURE 17-7 Gross image of the lung containing an irregularly marginated, gray-tan tumor mass with areas of hemorrhage and a “gritty” cut surface in a patient with a history of carcinosarcoma. |
METASTATIC TUMORS TO THE LUNG, HISTOLOGY
Histologically and cytologically, metastatic tumors to the lungs may mimic the histologic and cytologic features of their primary tumors; however, these histologic and cytologic features may not be specific. When it is unknown whether a lesion represents a primary lung tumor or a metastasis, features such as multifocality of tumor, pushing rounded tumor margin, lack of central fibrosis or elastotic scarring, prominent and diffuse lymphatic involvement, dirty necrosis, and a prominent lymphocytic component within the tumor are nonspecific features suggestive of metastasis.6 Some metastases have histologic features that give little guidance as to primary site of the tumor. Such is often the case with poorly differentiated or undifferentiated non-small cell carcinomas in the lung. There is also little histologic guidance found with squamous cell carcinomas
metastatic to the lung; their histologic characteristics significantly overlap and may be essentially identical regardless of primary site of tumor, be the primary site lung, cervix, skin, or head and neck, or another potential primary site (Fig. 17-8).
metastatic to the lung; their histologic characteristics significantly overlap and may be essentially identical regardless of primary site of tumor, be the primary site lung, cervix, skin, or head and neck, or another potential primary site (Fig. 17-8).
Related posts:
 Proposed Revisions to the Classification of Adenocarcinoma 5
Adenocarcinoma
Atypical Carcinoid Tumor
Update on Classification of Neuroendocrine Carcinomas
Multimodality Theranostics and Molecular Imaging in the Diagnosis and Treatment of Lung Cancer
Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia
Proposed Revisions to the Classification of Adenocarcinoma 5
Adenocarcinoma
Atypical Carcinoid Tumor
Update on Classification of Neuroendocrine Carcinomas
Multimodality Theranostics and Molecular Imaging in the Diagnosis and Treatment of Lung Cancer
Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


