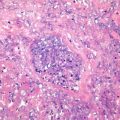
Fig. 10.1
Extrahepatic biliary adenoma: the adenoma cosists of multigrade slender papillary branches on the surface, with fibrovascular cores, and the papilla consists of cubic or columnar epithelial cells containing mucus
Tubular-papillary BDA consists of tubular glands and papillary structures, with each component accounting for more than 20%. Surgical resection is effective for the treatment of BDA . Dowdy et al. reviewed foreign literature and found 27 cases of BDA with complete pathological data from 1929 to 1960 [2], while Ming-yin Lan et al. (2012) analyzed the 17 cases of BDA reported at home and abroad from 1961 to 2011, including eight cases in upper part, one case in the middle part, and eight cases in the lower extrahepatic biliary system, showing that the male to female ratio was 5:12, the average age was 58.4 (21–73) years, and the clinical manifestations are nonspecific digestive and biliary symptoms.
Oshikiri et al. (2002) reported that glandular epithelium of papillary adenoma may contain atypical hyperplasia or focal carceration [3], and p53and Ki-67 staining can be carried out to evaluate the lesions. Tretiakova et al. (2012) reported that almost all of the extrahepatic biliary benign tumors, including BDA and low-grade dysplasia, were positive for CD10, with the number of positive stained cells ranging from 20 to 80%, and malignant tumors, including adenocarcinoma and high-grade dysplasia, were all CD10 negative, which can be considered as a key point in the differential diagnosis [4].
10.1.2 Granular Cell Tumor
10.1.2.1 Pathogenesis and Mechanism
Abrikossoff first reported granular cell tumor (GCT) in 1926, and in 1952, Coggins reported the first case of biliary GCT [5], also known as granular cell myoblastoma, which is a type of neurogenic tumor derived from Schwann cells based on the evidence in histology, immunohistochemistry, and electron microscopic observations. GCT is often found in the skin, subcutaneous tissues, tongue, breast, and gastrointestinal tract, while cases in the hepatobiliary system are rare with an incidence rate of less than 1% in all GCT. More than 70 cases of GCT in the extrahepatic biliary tree had been reported in the literature by 2012, accounting for less than 10% of biliary benign tumors [6, 7]. The tumor can show multicentric growth pattern, accompanied by GCT lesions in the gallbladder or skin.
10.1.2.2 Clinical Features
Foreign reports of granular cell tumor involve mainly the Negro population (60.5%) and young females (81%), with an average age of 33.9 (11–63) years. The clinical manifestations are similar to those of sclerosing cholangitis and cholangiocarcinoma, including abdominal pain (88%) and jaundice (53%). The lesions are often found in the junction of the cystic duct, common hepatic duct, and common bile duct [8], including common bile duct (58.1%), common hepatic duct (23.3%), cystic duct (14%), gallbladder, and duodenal ampulla (2.3%) [7]. Portal granular cell tumor can be similar to portal cholangiocarcinoma.
10.1.2.3 Gross Features
The lesions are often solitary without capsule, brownish yellow or yellowish white, and the average diameter is 1.6 (0.5–4) cm.
10.1.2.4 Microscopic Features
Tumor cells are arranged in sheets, acini, or clusters, with connective tissue separation. The tumor cells are polygonal or round in a larger size, rich in eosinophilic granular cytoplasm, with indistinct cell borders, and small and darkly stained nuclei (Fig. 10.2). These tumor cells can invade the whole layers of the bile duct wall, as well as nerve and small blood vessels in the biliary wall [7].
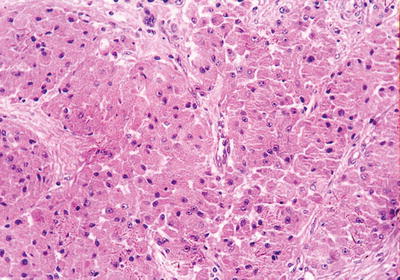
Fig. 10.2
Granular cell tumor of extrahepatic biliary: the tumor cells are arranged in acini, with abundant eosinophilic granular cytoplasm
10.1.2.5 Immunohistochemistry
The tumor is positive for S-100, GFAP, and NSE staining.
10.1.2.6 Electron Microscopic Observation
Large quantities of lysozyme granules in the cytoplasm can be observed.
10.1.2.7 Differential Diagnosis
Although there is no report of malignant GCT of the bile duct, we should also pay attention to this kind of tumor. Generally, malignant GCT should show corresponding pathological biological behaviors, including invasion of surrounding tissues and cellular atypia, mitotic figures, rapid growth, tumor diameter >4 cm, metastasis and recurrence, etc.
10.1.2.8 Treatment and Prognosis
GCT of the gallbladder or cystic duct can be treated with simple cholecystectomy, and GCT of pancreatic segment of extrahepatic bile ducts often needs to be treated with Whipple surgery, while postsurgical radiotherapy and chemotherapy are not necessary for benign GCT lesions.
10.1.3 Cystadenoma
Ninety percent of cystadenoma are found in intrahepatic biliary system, and extrahepatic biliary adenoma is rare with about 100 cases in the current literature. Ninety-five percent of cystadenoma are mucinous, and the rest are serous. The average onset age of the patients is 48–58 years, and 80% of the patients manifest as obstructive jaundice. The serum CA19-9 can be elevated. Thickened cystic wall displayed on imaging, with calcification and papilla in the septa of the cystic cavity, suggests malignancy of the tumor [9]. Grossly, the tumor is often a solitary, spherical, or round mass, cyst-solid in texture, and the section shows multilocular structures, containing mucus or serous fluid. The tumor grows and extends along the biliary lumen of 2.5–28 cm in size. Histologically, 80% of cystadenomas are characterized by a monolayer of cubic or columnar epithelium and underlying ovary stroma (Fig. 10.3). The patients are predominantly females. Ovary stroma can be positive for ER and PR. However, cystadenoma without ovary stroma is often found in the elderly with no significant gender difference. The stromal component is hyalinized collagen connective tissue [10]. The postsurgical recurrence rate of biliary cyatadenoma is 10%, which may develop into cystadenocarcinoma . Studies have shown that the prognosis of hepatobiliary cystadenoma with ovary-like stroma is better than that of cases without ovary-like stroma [11]. This kind of tumor should be differentiated from simple cyst, cystic hamartoma, intraductal papillary tumor of bile duct , etc.
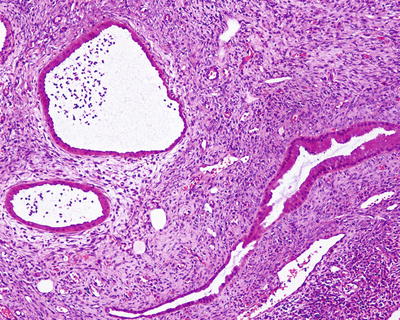
Fig. 10.3
Cystadenoma of extrahepatic biliary: the cystadenoma is characterized by a monolayer of cubic or columnar epithelium and underlying ovary stroma
10.1.4 Papillomatosis
Caroli first described multiple papillomatosis of bile duct in 1958, and there have been nearly 140 biliary cases up to now, the pathogenesis of which may be related to bile stimulation and chronic inflammation of the bile duct, including bile duct stones, Clonorchis sinensis, Caroli’s disease, ectopic pancreas, abnormal biliary tree, and primary sclerosing cholangitis [12]. Male patients are slightly more common with a male to female ratio of 2:1, and the common age range is 60–70 years. One case of the disease was found in the Department of Pathology, Eastern Hepatobiliary Surgery Hospital, Second Military Medical University, concerning a 54-year-old female, with multiple submucosal papillary lesions on the upper segment of common bile duct via choledochoscope, which was diagnosed as papillomatosis of the common bile duct based on the microscopic features (Fig. 10.4). Extrahepatic biliary papillomatosis may involve both the intrahepatic and extrahepatic biliary systems, and clinical manifestations are characterized as recurrent obstructive jaundice and cholangitis. ERCP examination is useful in establishing the diagnosis. Histologically, the tumor grows inward the biliary cavities with papillary structures and should be differentiated from canceration of papillomatosis or papillary adenocarcinoma based on the careful identification of the atypia of the tumor cells and the existence of biliary wall invasion. It has also been considered as a low malignant tumor according to its clinical and biological behaviors. Lee et al. (2004) suggested in a study that the canceration rate of biliary papillomatosis was as high as 83% [13]. Surgical resection is the preferred therapy; however, recurrence rate is high due to unresectable margin of the lesions or multi-lesion. Thus, for cases involving multigrade branches of bile ducts with high malignant potential, liver transplantation may be the best choice to improve the prognosis [14].
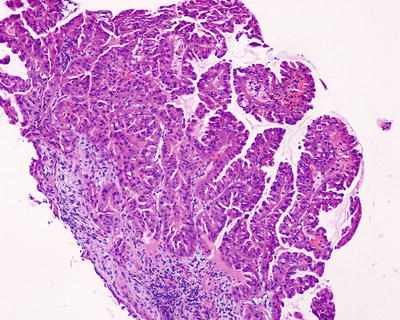
Fig. 10.4
Papillomatosis of extrahepatic biliary: the tumor grows inward the biliary cavities with papillary structures
10.1.5 Adenofibromyomatous Hyperplasia
Adenofibromyomatous hyperplasia has a low incidence in extrahepatic bile duct, and most of the cases are found in the Vater ampulla at the end of the common bile duct. Imaging shows irregularly thickened wall of the common bile duct, and the formation of tumor-like nodules can be diagnosed as adenomyoma. Histologically, it presents hyperplasia of submucosal glands and smooth muscles (Fig. 10.5). Muriel et al. (2009) reported one case of diffuse adenomyomatosis in the lower part of the common bile duct, extending a length of 4 cm, with microcysts of 1–3 mm in diameter on the cystic wall. The microscopic observation shows benign hyperplasia of glands with focal low-grade intraepithelial neoplasia [15]. Cases with atypia in the hyperplastic mucosal glands and obstructive jaundice should be differentiated from cholangiocarcinoma.
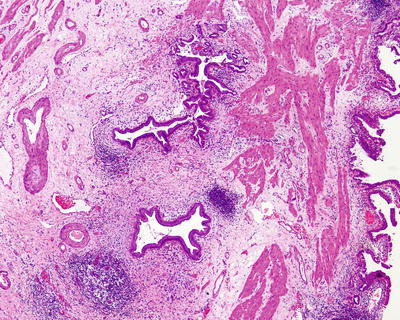
Fig. 10.5
Adenofibromyomatous hyperplasia of extrahepatic biliary: the lesion presents hyperplasia of submucosal glands and smooth muscles
10.1.6 Angioleiomyoma
Pönkä et al. (1983) reported one case of an 80-year-old female with a space-occupying lesion in the common bile duct via ERCP, which was pathologically confirmed as angioleiomyoma [16].
10.1.7 Leiomyoma
So far, five cases of leiomyoma have been reported in the literature [17], including three cases of common bile duct leiomyoma which were all located in the pancreatic segment of the common bile duct, possibly related to the existence of the circular smooth muscle or sphincter. The tumor is only a few millimeters in diameter, and no other special symptoms or signs are found apart from obstruction jaundice. Serum CA19-9, CEA, and AFP were negative.
10.1.8 Traumatic Neuroma
Traumatic neuroma is caused by tumor-like hyperplasia of the nerve and fibrous tissues in the injured bile duct wall, with varying components of the nervous tissues. It is often found in the residues of cystic duct after cholecystectomy. Herrera et al. (2009) reported 15 cases of traumatic neuroma in postsurgical extrahepatic biliary system after liver transplantation. The incidence rate of traumatic neuroma is 3.5% (15/428), and the lesions may originate in the common bile duct wall (type I) or the peripheral nerve tissue (type II) [18]. In addition, a few cases of neurofibromatous hyperplasia are found secondary to chronic cholecystitis.
10.1.9 Paraganglioma
Less than five cases of biliary paraganglioma have been reported in the literature, with the first case reported by Sarma et al. in 1980 [19]. Hitanant et al. (1984) reported a case of a 5 cm × 2 cm × 1.8 cm paraganglioma in the common hepatic duct which was surgically excised [20]. Caceres et al. (2001) reported one case of a 28-year-old female with surgically excised paraganglioma in the common bile duct, who manifested as right upper abdominal pain for more than 3 months, with normal serum catecholamine and no symptoms caused by biliary obstruction, and she showed good condition during the 6-year follow-up after the resection. Its microscopic features are similar to common paraganglioma, and the tumor consists of chief cells and supporting cells, forming cellular nests (cellular sphere), containing rich granular cytoplasm. Fibrous septa with abundant capillaries are found between these nests. Immunohistochemistry staining shows that the nest margin contains S-100-positive supporting cells containing neuroendocrine particles which can be found in electron microscopic images [21]. Malignant biliary paraganglioma has been reported in rare cases and should be carefully distinguished.
10.1.10 Neurofibroma
Neurofibroma is rare, and less than 20 of cases have been found in foreign literature so far [22]. Most of the tumors are associated with neurofibromatosis type 1 gene (NF1), but there are also reports of primary neurofibroma in the common bile duct [23]. Sukanta (2011) et al. reported one case of a 47-year-old female with neurofibroma in the common bile duct which was surgically excised. A lesion of 2 cm×2.5 cm of the common bile duct was found, causing stenosis and resulting in progressive obstructive jaundice. Two cases of extrahepatic biliary neurofibroma have been diagnosed in the Department of Pathology, Eastern Hepatobiliary Surgery Hospital, Second Military Medical University, concerning a 57-year-old male with a 2 cm × 1.8 cm lesion and a 68-year-old female with a 0.4 cm × 0.5 cm lesion, respectively. The tumors are grossly solid, grayish white, and nodular, while the microscopic observation shows that they are similar to common neurofibroma, with spindle tumor cells in wavy, spiral, or fence-like arrangement, and no atypia is observed. Immunohistochemistry shows that the tumors are positive for neural markers such as S-100 (Fig. 10.6).
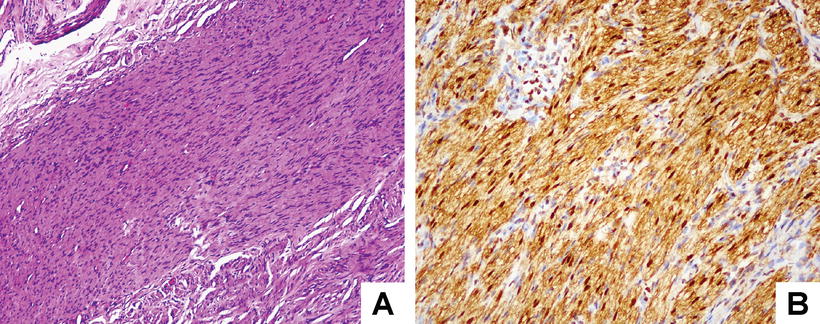
Fig. 10.6
Neurofibroma of extrahepatic biliary: (a) spindle tumor cells are in wavy, spiral, or fence-like arrangement and no atypia is observed; (b) immunohistochemistry shows that the tumor is positive for neural marker S-100
10.1.11 Inflammatory Myofibroblastic Tumor
Extrahepatic biliary inflammatory myofibroblastic tumor (IMT) is a special type of inflammatory pseudotumor , which is more prone to present invasive behaviors, or is an independent type of lesions containing myofibroblasts. Its histological features are the same with those of intrahepatic IMT [24], and cases with positive expression of anaplastic lymphoma kinase (ALK) concern more young patients with a good prognosis. On the contrary, ALK negative cases are more common in elder patients with higher rate of metastasis. Biliary IMT lesions are often benign in nature; however, Kim et al. (2011) reported one case of portal IMT with high invasiveness, consisting of atypic tumor spindle cells, with common mitotic figures, and the myofibroblasts were positive for SMA and vimentin. Metastasis in the right chest wall was found 4 months after surgery, and malignant spindle cells were found in biopsy [25]. Thus, invasive IMT should be identified in the diagnosis of IMT .
10.1.12 Inflammatory Pseudotumor
Extrahepatic biliary inflammatory pseudotumor (IPT) has been reported in more than ten cases, and its histological features are the same with intrahepatic IPT. It consists of chronic inflammatory cells and hyperplastic fibrous connective tissues, causing biliary obstruction which leads to jaundice clinically, similar to the manifestation of portal cholangiocarcinoma or extrahepatic cholangiocarcinoma (ECC) . Blanton et al. (2011) reported one case of a 20-year-old female with persistent jaundice. Abdominal CT showed dilatation of intrahepatic bile ducts, with obscure soft tissue densities in the portal area. ERCP demonstrated that an irregular stenosis was shown in the middle of the common hepatic duct, and choledochoscopic observation showed ulcerative changes. Cytological and choledochoscopic biopsy showed no definite malignant lesions. Postsurgical pathological examination confirmed the composition of spindle myofibroblasts, plasma cells, lymphocytes, eosinophilic granulocytes, and neutrophils, leading to obstruction and thickened wall of the common bile duct (incorrect, reference resource was not found), suggesting the possible existence of IPT in suspected cases of extrahepatic biliary malignant tumor. Some patients have IgG4-related sclerosing cholangitis in the background of autoimmune pancreatitis, with marked elevation of serum IgG4, and immunohistochemistry shows the presence of large quantities of IgG4-positive plasma cells. And these patients are sensitive for hormone therapy .
10.1.13 Gastrinoma
Gastrinoma is common in the pancreas and duodenum, while cases involving the extrahepatic biliary (including the common bile duct and common hepatic duct) are rare with only about ten cases reported in the literature, suggesting the possible origination in the stem cells of the ventral pancreatic bud. It manifests clinically as typical Zollinger-Ellison syndrome, but biliary obstruction or jaundice is rare. The tumor can form a mass larger than 1 cm in diameter on the biliary wall. Immunohistochemistry shows that it is positive for CgA and Syn and positive or negative for gastrin. Hepatic MRI and CT or single photon emission computed tomography of somatostatin receptor are helpful to exclude metastatic tumors originating from the liver or the “gastrinoma triangle.” Early detection and surgical resection receive a good prognosis, with disappearance of clinical symptoms and return to normal serum gastrin [26].
10.1.14 Eosinophilic Cholangitis
According to statistics, about 10% of tumors causing portal stenosis are confirmed as benign tumors after surgical resection, which are also known as malignant masquerade. For instance, eosinophilic cholangitis in the common bile duct shows similar clinical and imaging features to cholangiocarcinoma. Dubay et al. (2010) reported one case of a 29-year-old female with upper abdominal pain and other digestive symptoms, and magnetic resonance cholangiopancreatography showed a 2 cm long stenosis in the middle of the common bile duct. Endoscopic ultrasound images showed an 8 mm focal wall thickening of the common bile duct, which was reactive bile duct epithelium shown in puncture examination, without tumor cells. The pathological examination showed that the thickened common bile duct wall contains infiltration of a large number of mature eosinophilic inflammatory cells and formation of eosinophilic abscess, with proliferated fibroblasts, and the pathological diagnosis was eosinophilic cholangitis. The disease often can be accompanied by increased eosinophilic granulocytes in the blood, and the differential diagnosis needs to be made to exclude the use of steroid hormone, parasite infection, and allergic reaction [27].
10.1.15 Neurilemmoma
Neurilemmoma derives from Schwann cells, also known as Schwannoma, and the predilection site is the digestive tract including the stomach, colon, and esophagus, while cases involving extrahepatic biliary system are rare with 15 cases reported in the foreign literature by 2012 [28]. Domestic cases of extrahepatic biliary neurilemmoma including those reported by our hospital can also be found [29]. The patients present a male to female ratio of 1:4, and an age range of 15–64 years (44 years old on average), and most of them (11/15) have symptoms of obstructive jaundice. The tumor originates in the Schwann cells of peripheral nerve of the biliary wall, with a capsule, and intratumorous hemorrhage, hyaline degeneration, and cystic degeneration can be found in some cases. The tumor consists of two main structures. Antoni A type contains densely distributed spindle or oval cells in the palisade and plexiform form. Antoni B type consists of loose and disordered tumor tissues in the myxoid matrix with edema. It is currently believed that neurilemmoma deriving in the digestive tract is mainly Antoni A type without mutations of neurofibromatosis type 2 gene (NF2) [30]. And it should be differentiated from neurofibroma, gastrointestinal stromal tumor , and leiomyoma . Immunohistochemistry shows that it is positive for S-100 and vimentin and negative for CD117 and CD34. Surgical resection prompts a good prognosis.
10.1.16 Heterotopias
Heterotopias of gastric mucosa into the extrahepatic biliary system are the most common type, and nine cases have been reported in the foreign literature with a male to female ratio of 2:1 and an average age of 37 (3–83) years. Of which six cases are found in the location near the junction of common bile duct and cystic duct, while the rest are located in the left hepatic duct, portal bile duct, and ampulla. The lesions are 3–25 mm in size, and the patients may present jaundice, abdominal pain, etc [31]. In addition, other ectopic tissues include pancrea, duodenum, accessory liver, adrenal gland, and thyroid gland, and imaging shows biliary occupying lesions. In histology, these ectopic tissues consist of normal parenchymal cells of the primary organs. However, malignancy has also been discovered in them and should be carefully observed when necessary.
Moreover, other benign non-epithelial tumors of the extrahepatic bile duct include lipomyoma, lymphangioma, angioma, melanoma, etc. The histomorphology is similar to those in soft tissues, which need not be repeated here.
10.2 Malignant Tumors of Extrahepatic Bile Duct
10.2.1 Extrahepatic Cholangiocarcinoma
10.2.1.1 Pathogenesis and Mechanism
Cholangiocarcinoma is usually abbreviated for extrahepatic cholangiocarcinoma (ECC ) . Extrahepatic bile ducts include the left and right hepatic duct, common hepatic duct, cystic duct, and common bile duct, and according to the orientation of the common bile duct and the relationship with the surrounding organs, it can be divided into superior-duodenum, posterior-duodenum, and pancreatic and duodenal wall segments. The incidence of ECC is low and knowledge on ECC is far more less than that on intrahepatic cholangiocarcinoma. And 50–75% of the tumors are found in the upper one third of extrahepatic bile ducts including the portal area, and the lesions are more common in the confluence of thecommon bile duct, hepatic duct, and cystic duct. Cases in the middle one third (segment of the common bile duct between the cystic duct and the inferior margin of duodenum) account for 10–25%, while cases involving the lower one third segment (segment of the common bile duct between the inferior of duodenum and Vater ampulla) account for 10–20%. The predilection age is 60–70 years, and no gender difference is found related to the incidence. According to the domestic joint analysis on the 1979 autopsy cases of malignant tumors conducted by 38 departments of pathology of medical university, ECC accounted for only 0.07%. And according to the statistics provided by Shanghai Cancer Research Institute, male and female standardized incidences of gallbladder carcinoma and cholangiocarcinoma from 1978 to 2000 had been raised from 1.6/100000 and 2.3/100000 to 3.8/100000 and 5.4/100000, which were 2.46/100000 and 3.77/100000 in 2005, respectively, suggesting a drop in the incidence. Furthermore, it has been reported that new cases of gallbladder carcinoma and extrahepatic cholangiocarcinoma reached about 9810 in the USA in 2012, with 3200 death cases. And statistics of related data from 1985 to 2005 showed that the incidence of ECC in males and females were 1.1/100000 and 0.7/100000, respectively [32, 33].
The pathogenesis of ECC remains unclear, and the etiology may include ulcerative colitis (the incidence of which may be 9–21 times higher than that in normal population), primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PSC), and several congenital biliary malformations such as congenital choledochocyst, congenital cyst of common bile duct (CCC), congenital malformation of the biliary tract, Carroli’s disease, congenital hepatic fibrosis, polycystic liver and anomalous pancreatico-choledocho-ductal junction, biliary stones, parasitic infections (such as Clonorchis sinensis), exposure to chemical carcinogens, etc. (such as thorium anhydride), and patients with these lesions should be followed up closely. Other risk-increasing factors include diabetes, smoking, drinking, and infection of HBV/HCV [34–36]. Wang et al. (2011) made a meta-analysis on ECC , showing that 28–50% of the patients were (40% on average) p53 positive, the higher expression levels of which were associated with poorer staging of the tumor and histological type, vascular invasion, and lymphatic metastasis [37]. Chung et al. (2009) examined the tissue microarray of 221 cases of ECC and found elevation of phosphorylation AKT and mTOR levels [38], as well as reduction of PTEN expression in ECC , suggesting the possible application of PTEN, PTEN/p-AKT, and PTEN/p-mTOR as indicators for evaluation of the prognosis of ECC . Kawamoto et al. (2007) discovered that ECCs contain amplification of HER-2 gene (21.4%) and positive expression of the protein (31.3%); the practical significance needs further confirmation [39].
Nitta et al. (2014) found that the high expression rate of Ambra1, an autophagy protein, in cholangiocarcinoma was 71%, and the remaining 29% showed low expression. Ambra1 expression and lymphatic metastasis (P = 0.0391) or poor postsurgical 2-year overall survival rate (P = 0.0209) were significantly correlated, suggesting that autophagy played an important role in the invasive growth process of cholangiocarcinoma [40]. Nitta et al. (2014) found that epithelial-mesenchymal transition (EMT) is an important phenotype feature for cholangiocarcinoma and EMT associated markers showed significant correlation with the poor prognosis of cholangiocarcinoma, including E-cadherin (P = 0.0208), N-cadherin (P = 0.0038), and S-100A4 (P = 0.0157) [41].
10.2.1.2 Clinical Features
Wen-bing Wang et al. (2008) published a group of data showing that ECC patients were predominantly male, accounting for about 69% in all cases, while females accounted for only 31%, and the age range was 30–82 years with an average age of 58.6 years. Jaundice was the most common clinical symptom, which appeared earlier than that in gallbladder carcinoma with progression or volatility, found in 81.4% of all the cases. Other clinical manifestations included upper abdominal pain (29.2%), upper abdominal distension and discomfort (13.7%), itch (9.3%), fever (8.1%), and lack of appetite (5%) [42]. Laboratory tests showed elevation of tatal bilirubin and marked elevation of serum CEA and CA19-9. A total of 563 cases of surgically excised ECC were diagnosed in the Department of Pathology, Eastern Hepatobiliary Surgery Hospital, the Second Military Medical University from 2007 to 2014, and the average age of the patients was 59.1 (13–82) years, including 359 males and 204 females, with a male to female ratio of 1.76:1.
There are two basic points of the imaging features of ECC : ① biliarty obstruction caused by tumor lesions and ② direct signs of the tumor and the biliary invasion in imaging. The X-ray examination shows soft Rattan-like expansion of the bile ducts proximal to the obstruction, with irregular concentric or eccentric stenosis in the obstructive bile duct. And endoscopic retrograde cholangiopancreatography (ERCP) is very useful for the location of the ECC lesions, while endoscopic ultrasound has a diagnostic accuracy of 86% for detection of the infiltration depth of the ECC . Combined application of ERCP and percutaneous transhepatic cholangiography (PTC) can show the complete superior and inferior margins of the tumor, which is of crucial significance in determining the size, region, and treatment regime of the tumor; however, it may cause hemorrhage, bile leakage, biliary tract infection, pneumothorax, and other complications, due to its invasiveness. Magnetic resonance cholangiopancreatography (MRCP) is noninvasive, nonradioactive with arbitrary tomography and high resolution for soft tissues, etc., and the tumor is mainly the signal of soft tissue masses or thickened biliary wall, with irregular biliary stenosis. It is of important value in detection of the infiltration into the surrounding tissues and lymphatic metastasis, due to its good capacity in angiography, especially the advantage in the simultaneous imaging of both the superior and inferior segments of the obstructive bile duct after 3D reconstruction with high sensitivity and specificity. With the application of new technology of high-resolution ultrasound, detection rate of extrahepatic biliary cholangiocarcinoma can be up to 90.16% via color Doppler ultrasound [43].
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


