Effects of gonadal steroids on the hypothalamus during gonadal formation [4]
Disorders of androgen to estrogen conversion [5]
Receptor disorders
Aromatase changes [6]
Gender identity is developed as a result of the interaction between the developing brain and gonadal steroids from the 8th to 12th gestational week. Swaab and Hofman [7] found a gender-specific difference between the volume of the suprachiasmatic nucleus and the nuclei striae terminalis. The latest studies from Prince Henry’s Institute in Australia implied a longer androgen receptor gene, leading to less effective circulating testosterone, undermasculinization and a brain more similar to a female brain in MFTs. This study was criticized by the fact that in some other disorders with changes in androgen receptors no similar changes in psychic gender were found. Trying to make a contribution to examining the etiology of transsexualism, our team provided data on finger lengths in transsexuals [8].
6.3 Incidence
Since 1966, many studies have referred to the incidence of transsexualism. The ratio between MFTs and FMTs has varied, depending on surgeons’ willingness to perform the operation. Because male-to-female surgery is less complicated, there have been more MFTs. In countries with highly specialized surgeons, such as Serbia, the number of transsexuals has been the same (male-to-female and female-to-male) [9]. In Table 6.2, the incidence of transsexualism is shown.
Table 6.2
Incidence of transsexualism around the world
Author | Year | Country | Ratio MF:FM |
|---|---|---|---|
Benjamin | 1966 | USA | 6:1 |
Eklund | 1988 | Netherlands | 3:1 |
Godienski | 1988 | Poland | 1:5.5 |
Ross | 1981 | Australia | 9:1 |
Garrels | 2000 | Germany | 1.2:1 |
Vujovic | 2009 | Serbia | 1:1 |
In some studies, the number of patients was too small. In human biology the incidence of many disorders is the same in males and females and it would be difficult to explain such a high difference in ratio, except with some technical details regarding the operations.
6.4 Diagnosis
A team of three highly educated psychiatrists in the field of sexual disorders confirm the diagnosis after 1 year or more of follow-up. They have to exclude many psychiatric disorders such as transvestitism, homosexuality etc. After that the endocrinologist examines the patient, detects the karyotype and carries out hormonal analysis. It is necessary to take blood samples in MFTs for follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin, estradiol, progesterone, testosterone, SHBG, 17 OH progesterone, free thyroxine, thyroid-stimulating hormone (TSH), and cortisol. In FMTs on day 7 of the menstrual cycle (for those younger than 30 years of age) blood samples are taken for FSH, LH, prolactin, estradiol, testosterone, androstenedione, dehydroepiandrosterone sulfate (DHEAS), 17 OH progesterone (to exclude congenital adrenal hyperplasia), fT4, TSH, cortisol and on day 21 progesterone is measured. According to these results endocrine diseases mimicking transsexualism can be excluded such as androgen-secreting tumors, congenital adrenal hyperplasia, pseudohermaphroditism of other different origins, and some other endocrine diseases, such as thyroid and adrenal gland diseases. A complete internal examination and an ultrasound of the gonads (ovaries or testis) and breasts are obligatory.
After confirming diagnosis from the endocrine point of view therapy regarding the characteristics of the opposite sex can be initiated. Sperm of MFTs can be frozen if desired and FMTs can store their follicles in case they want to have a biological child later on.
6.5 Therapy
The aim of the therapy is to help a patient to look like a person they feel that they can depend upon to provide normal sexual function and work abilities, and to determine the dosage of the therapy individually.
6.5.1 Male to Female Therapy
Before the operation and 6 months later oestradiol ampoules at 10 mg are given intramuscularly within a 7- to 10-day interval with ciproterone acetate (50 mg daily orally). Micronized progesterone is added 7 days a month (100 mg) after 6 months of therapy. From 6 months after the operation estroprogestagen therapy is initiated orally and it is necessary to continue throughout life. Ciproterone acetate is reduced to 25 mg, according to hirsutism status. The effects of estrogen, progestogen and antiandrogen therapy on body shape is shown in Table 6.3. There are many reasons for adding progesterone (Table 6.4).
Table 6.3
 Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Hormonal Contraceptives: Progestogen and Thrombotic Risk
Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Hormonal Contraceptives: Progestogen and Thrombotic Risk
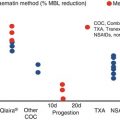 Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
Cardiovascular Prevention at the Menopausal Transition: Role of Hormonal Therapies
Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
Cardiovascular Prevention at the Menopausal Transition: Role of Hormonal Therapies
 Low Malignant Potential Tumors
Low Malignant Potential Tumors
 Disorders of the Menstrual Cycle During Adolescence
Disorders of the Menstrual Cycle During Adolescence




Changes in symptoms and signs during therapy for male to female transsexuals (MFTs)
Related posts:
Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Hormonal Contraceptives: Progestogen and Thrombotic Risk
Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
Cardiovascular Prevention at the Menopausal Transition: Role of Hormonal Therapies
Low Malignant Potential Tumors
Disorders of the Menstrual Cycle During Adolescence
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
