SYNDROMES OF REAL OR APPARENT MINERALOCORTICOID EXCESS NOT CAUSED BY ALDOSTERONE
Part of “CHAPTER 80 – HYPERALDOSTERONISM“
CLINICAL FEATURES AND PATHOPHYSIOLOGY
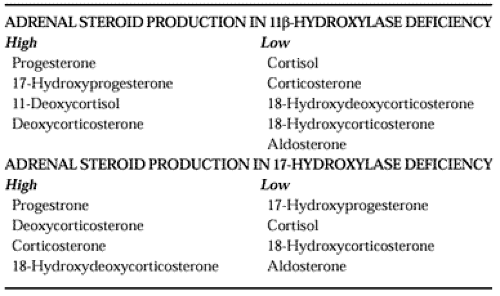
Occasionally, patients may have features of mineralocorticoid excess (hypokalemic alkalosis, suppressed plasma renin activity, and hypertension) but plasma aldosterone concentrations that are low or undetectable (see Table 80-1). Some of these patients
have increased production of other mineralocorticoids, such as deoxycorticosterone or corticosterone, as a result of 11β-hydroxylase deficiency or 17-hydroxylase deficiency, respectively (Table 80-3; see Chap. 77); others do not overproduce any of the known adrenal steroids. Still others accumulate an abnormal amount of cortisol in renal tubule cells because of 11β-hydroxysteroid dehydrogenase deficiency that leads to increased occupancy of mineralocorticoid receptors by cortisol.53
have increased production of other mineralocorticoids, such as deoxycorticosterone or corticosterone, as a result of 11β-hydroxylase deficiency or 17-hydroxylase deficiency, respectively (Table 80-3; see Chap. 77); others do not overproduce any of the known adrenal steroids. Still others accumulate an abnormal amount of cortisol in renal tubule cells because of 11β-hydroxysteroid dehydrogenase deficiency that leads to increased occupancy of mineralocorticoid receptors by cortisol.53
 |
In Liddle syndrome, increased renal tubular reabsorption of sodium and secretion of potassium presumably are independent of stimulation by a mineralocorticoid because they are unaffected by treatment with spironolactone.54 The cause of Liddle syndrome is mutations in the βsubunit of the epithelial sodium channel.55
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


