Chapter 13 Survivorship and Late Effects
General Considerations
The QUANTEC Initiative
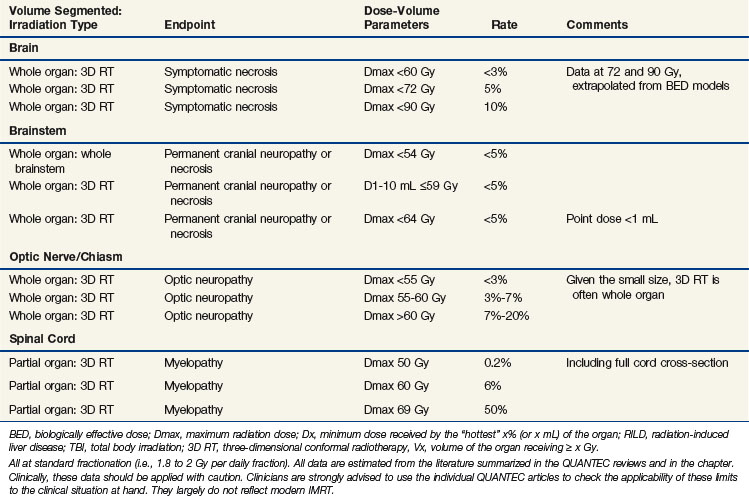
This chapter will summarize and expand upon several reviews published as a special issue in the International Journal of Radiation Oncology Biology Physics (volume 76, issue 3, Supplement), all of which were written as part of the Quantitative Analysis of Normal Tissue Effects in the Clinic (QUANTEC) initiative. QUANTEC arose from a proposal from the Science Council of the American Association of Physicists in Medicine (AAPM) to revise and update guidelines published by Emami in 1991.1 QUANTEC’s goals are (1) to provide a critical review of the current literature on quantitative dose-response and dose-volume relationships for clinically relevant normal-tissue endpoints; (2) to produce practical guidelines to allow reasonable toxicity risks based on dose-volume parameters; and (3) to identify future research initiatives. Using the QUANTEC reviews as a backbone, this chapter will focus on recently published data relevant to late toxicity from radiation, with an emphasis on dose-volume metrics. Key summary points of the QUANTEC reviews are briefly summarized at the end of each section, and the QUANTEC reviews are referenced at the end of each section. Table 13-1 summarizes the dose-volume metrics that are supported by the literature; this table was modified from the one published in the QUANTEC issue.2
Although the QUANTEC initiative and associated reviews address a broad range of issues relating to normal tissue damage, this chapter will focus on late toxicity after an initial course (i.e., excluding re-irradiation) of conventional radiation (i.e., excluding hypofractionated regimens).3 Studies relating three-dimensional dose/volume metrics to clinical outcomes will be the main subject.
Nervous System: Brain
Dose-Volume Data
Recent prospective studies in adults have shown that partial (and limited) brain irradiation in the dose range of 50 to 60 Gy causes minimal to no discernible effect on memory and cognition.4–9 However, another recent study has suggested that patients undergoing partial brain irradiation for low-grade glioma, versus patients who do not undergo irradiation, are at greater risk for neurocognitive deficits, particularly in attention, executive functioning, and information processing.10 More detailed studies, correlating neurocognition with susceptible regions within the brain, are needed. Certainly, ample data suggest that the volume of brain that is irradiated is a factor in the degree of radiation-associated neurocognitive decline (with whole brain irradiation causing more serious deficits).11 In adult patients who have received whole brain irradiation, neurocognitive decline is well described. However, the degree to which brain irradiation (versus factors such as surgical or chemotherapeutic treatment, the presence of hydrocephalus or comorbid illnesses, and tumor progression) may affect neurocognitive function is not clear.9,12,13
For children, younger age at irradiation and larger irradiated volumes (with higher doses having a greater impact) are associated with objectively worse neurocognitive function.14–17 For example, central nervous system prophylaxis for acute lymphoblastic leukemia with 24-Gy whole-brain irradiation in addition to intrathecal methotrexate (versus methotrexate alone) results in a median 13-point IQ reduction at 5 years after irradiation as well as poorer academic achievement and self-image and greater psychological distress at 15 years.18 Lower risks are associated with lower doses of 14 to 18 Gy.19–21 For medulloblastoma, increasing the brain dose in the 18- to 36-Gy range has been correlated with greater neurocognitive decline.14–16,22,23 Girls are observed to be more vulnerable to injury than boys.24 Reported toxicities are lower (or not detected) when 14 to 18 Gy is used.6–8 Radiation necrosis can occur in any part of the brain. Although there may be regional variations of susceptibility within the brain related to differences in vascularity, glial cell population, and so on, data on this topic are sparse, and it is generally believed that location does not generally affect susceptibility to necrosis. However, damage to specific regions, such as the brainstem, is more likely to cause symptoms. There is a paucity of data correlating dose-volume parameters with the risk of radiation necrosis with conventional fractionated therapy, though many studies have documented an association of fraction size with the risk of necrosis.
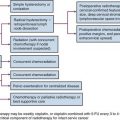
In a study from Queen Elizabeth Hospital in China, 1008 patients with nasopharyngeal cancer, treated before 1985, received 45.6 to 53.2 Gy in 3.8-Gy fractions, 50.4 Gy in 4.2-Gy fractions, or 60 Gy in 2.5-Gy fractions.25 The 10-year risk of temporal lobe necrosis was 18.6% in those treated with 4.2-Gy fractions versus less than 5% for the other dose schemes (p <.001). A multiinstitutional Chinese study examined 1032 patients with nasopharyngeal cancer treated after 1990 with one of several fractionation schemes (mostly 2- to 3.5-Gy fractions, though one scheme used a 1.6-Gy twice-daily component).26 The 5-year actuarial incidence of necrosis ranged from 0% (after 66 Gy in 2-Gy fractions) to 14% (after 2.5 Gy × 8 followed by 1.6 Gy twice daily to 71.2 Gy). In both of the above-mentioned studies, the combination of total dose and dose per fraction significantly affected the risk; a shorter overall treatment time and twice-daily fractionation also increased the risk. A Chinese study comparing 71.2 Gy in 1.6-Gy twice-daily fractions versus 60 Gy in 2.5-Gy fractions was terminated early because of excessive neurologic toxicity, including temporal lobe toxicity, in both arms. The risk of toxicity was greater and the interval to developing toxicity was shorter, with the twice-daily regimen.27 In another Chinese study, 27% of patients receiving an accelerated hyperfractionated regimen (64 Gy in 1.6-Gy twice-daily fractions) versus 0% of patients receiving hyperfractionated irradiation (70.8 Gy in 1.2-Gy twice-daily fractions) developed symptomatic radiation necrosis.28
Radiation necrosis has also been studied in patients with primary brain tumors. The risk is dose dependent, with doses of less than 50 Gy rarely causing necrosis.29–31 In patients treated for brain metastases, there was a low (<2%) risk of necrosis developing after 1.6 Gy twice daily to the whole brain (32 Gy), followed by a boost to 54.4 to 74.4 Gy, and no necrosis was seen after a boost to 48 Gy.32,33
Summary and Other Key Points from the QUANTEC Review34
A high level of evidence to quantify the risks of radiation-induced brain injury is lacking. For brain necrosis, the brain appears to be especially sensitive to fraction size in excess of 2 Gy and to twice-daily fractionated treatment. Symptomatic necrosis is uncommon with doses of less than 60 Gy with conventional (1.8- to 2-Gy) fractionation, though the risk increases with increasing dose (see Table 13-1). More detailed studies correlating neurocognition with susceptible regions within the brain are needed. Long-term (>5 years) follow-up is necessary to best assess neurologic and cognitive decline. For children, younger age and higher whole brain dose strongly correlate with cognitive decline. Future studies should provide a clear definition of toxicity and reported actuarial rates (as opposed to crude rates) that can be correlated with detailed normal brain dose-volume metrics.
Nervous System: Brainstem
Dose-Volume Data
Several institutions have published their dose-volume constraints for the brainstem, most of which have not reported any brainstem toxicity. These constraints for patients undergoing external beam radiation therapy for head and neck cancer include a V60 of less than 5 mL, V65 less than 3 mL,35 V55 less than 0.1 mL,36 D1 less than 54 Gy,37 and maximum less than 50 Gy38; and for patients undergoing proton or combined proton/photon therapy for base of skull lesions include less than 63 to 64 Gy CGE (cobalt Gray equivalent) to the brainstem surface and 53 to 54 CGE to the brainstem center.39–42
Some patients in these studies received a maximum brainstem dose of 66 to 68 CGE (greater than the desired constraints) in order to adequately treat the tumor.39,41,42 In one study, the dose constraint of 63 CGE to the brainstem surface and 54 CGE to the brainstem center was “relaxed” in 38% and 17% of patients, respectively, with no reported neurologic toxicity. In these patients, the volume receiving a dose above the threshold dose was 0.2 mL and 1.2 mL for the brainstem surface and center, respectively.41 In another study, two of four patients developing neurologic toxicity received maximal doses in excess of 64 Gy CGE to the brainstem surface and 53 CGE to the brainstem center.42
In an analysis of 367 patients from Massachusetts General Hospital, an increased risk of late toxicity was associated with the maximal delivered dose (>64 CGE), V50 (>5.9 mL), V55 (>2.7 mL), V60 (>0.9 mL) and a history of diabetes, hypertension, and more than two surgical procedures of the base of the skull, on univariate analysis.43,44 On multivariate analysis, only the V60 and a history of diabetes and more than two surgical procedures remained significant. A V60 of less than 0.9 mL versus more than 0.9 mL resulted in toxicity-free survival rates of 96% versus 79% (p = .0001), and on multivariate analysis resulted in an 11.4 risk ratio (p = .001). In a recent study from St. Jude Children’s Research Hospital on 68 patients with infratentorial ependymoma, several interrelated variables were associated with brainstem injury, including tumor volume (and, therefore, radiation volume), surgical morbidity, male gender, younger patient age, and cerebrospinal fluid shunting. The radiation dose was homogeneous between 54 and 59.4 Gy.45
In a study of 40 patients undergoing IMRT for meningioma, one patient developed fatal brainstem necrosis after receiving a maximum dose to the brainstem of 55.6 Gy, with 4.74 mL exceeding 54 Gy.46 This demonstrates that other poorly understood factors likely increase the risk of brainstem toxicity because this dose constraint would be considered acceptable in most of the studies referenced above.
Nervous System: Spinal Cord
Dose-Volume Data
It is well-accepted that the spinal cord can tolerate 45 to 50 Gy with conventional fractionation, though the TD5 (tolerance dose with 5% injury) is most likely much higher. The spinal cord is generally limited to 45 to 50 Gy because the anticipated risk of cord injury must be very low to be clinically acceptable. In an analysis of several studies, Schultheiss calculated the probability of cervical cord myelopathy after full cross-sectional irradiation as 0.03% after 45 Gy, 0.2% after 50 Gy, and 5% after 59.3 Gy.48 The thoracic spinal cord was calculated to be less sensitive than the cervical spinal cord (although because of the dispersion of data, a good fit could not be obtained). This model does not incorporate spinal cord volume, and this might be acceptable given the “series” nature of the cord. Nevertheless, Schultheiss cautions that long lengths of cord, concomitant chemotherapy, and other factors may increase the risk.
Little data exist exploring the dose-volume tolerance of the spinal cord. No spinal cord toxicity was reported in a study in which the V50 was less than 0.1 mL36 or in another study in which the D1 was less than 45 Gy.37 Massachusetts General Hospital recently studied 85 patients treated to the cervical spinal cord in the range of 45 to 59.4 Gy (1.5-Gy equivalent fractions) equivalent uniform dose (EUD), 42- to 57.5-Gy maximal dose to the cord center, and 57- to 74-Gy maximal dose to the cord surface.49 Fifteen percent of these patients experienced Lhermitte’s syndrome (self-limited transverse myelitis, with symptoms of electric shock-like sensation most notable with neck flexion), and 5% developed objective neurologic findings at or below the cord level treated. Toxicity was not significantly correlated with cord length, cord volume, maximal dose to the cord center, maximal dose to the cord surface, or effective uniform dose. The authors conclude that an EUD to the cervical cord of 60 Gy in 1.5-Gy fractions or 52.5 Gy in 2-Gy fractions is safe.
Nervous System: Optic Nerves and Chiasm
Organ Function and Clinical Significance
It is well-accepted that the entire system of optic nerves and the chiasm may be treated to 54 Gy using conventional fractionation with minimal risk of late visual toxicity, though lower doses can result in other ophthalmologic toxicity.51 In a study from M.D. Anderson Cancer Center (MDACC) in which 219 patients were treated before three-dimensional irradiation was available, 10-year actuarial rates of optic neuropathy were 0%, 3%, and 34% for 43 to 49 Gy at approximately 1.9 Gy per fraction, 50 to 60 Gy at approximately 2.1 Gy per fraction, and 61 to 76 Gy at approximately 2.2 Gy per fraction, respectively. Chiasm damage was similar, with rates of 0%, 8%, and 24% for 15 to 49 Gy at approximately 1.5 Gy per fraction, 50 to 60 Gy at approximately 2 Gy per fraction, and 61 to 76 Gy at approximately 2.1 Gy per fraction, respectively.52 Greater total dose as well as larger fraction size affected risk.53–56 With three-dimensional planning, small volumes of optic nerve and chiasm may tolerate higher doses.
Dose-Volume Data
Several institutions have published their dose-volume constraints for the optic nerves and chiasm, with most not reporting any neurologic visual toxicity. These constraints for patients undergoing external beam radiation therapy for head and neck cancer include V55 of less than 0.1 mL of the optic nerves and chiasm,36 D1 of less than 54 Gy for the optic nerves, and D1 of less than 45 Gy for the optic chiasm37 and a maximum of less than 54 Gy to the optic nerves and 52 Gy for the chiasm. For patients undergoing proton or combined proton/photon therapy for base of skull lesions, doses include less than 55 to 56 GGE40–42 or less than 60 Gy CGE39 to the optic nerves and optic chiasm.
Several studies have reported ophthalmologic toxicity after irradiation. In a study from the University of Florida, the optic nerve dose (defined as the minimum dose delivered to one-third of the optic nerve) in patients who developed optic neuropathy was 50.4 to 79 Gy (median, 68 Gy).56 In a University of Michigan study,57 seven patients developed ophthalmologic toxicity: one patient received a chiasm maximum of 59.5 Gy, and six patients received an optic nerve maximum of 47.5 to 75.5 Gy (average, 63 Gy). Moderate to severe optic nerve complications (four patients) were associated with doses of more than 64 Gy. In one study, four patients developed ophthalmologic toxicity; three had received a maximal dose of 56 to 62 CGE to the optic chiasm/nerves and one had received a maximum dose of more than 62 CGE. In two studies, bilateral visual loss occurred, with no evidence of tumor progression 8 months after conventional radiation; in one study, the prescribed target dose was 49.3 Gy (maximum dose, 56.1 Gy; chiasm maximum dose not reported, but <1 mL received >45 Gy),58 and in the other study, the chiasm maximum dose was less than 58 CGE.40
Some patients tolerate a maximum optic nerve or chiasm dose of more than 60 Gy or more than 63 to 69 CGE.38,39,41,42,57 This demonstrates that other poorly understood factors likely increase the risk of optic nerve and chiasm toxicity. An optic nerve maximum dose of more than 80 Gy and a chiasm maximum dose of more than 70 Gy were tolerated in some patients in the University of Michigan study discussed above.57 In another study, the dose constraint of 56 CGE to the optic nerve and chiasm was “relaxed” in 28% and 48% of patients, respectively, with no reported visual toxicity. In these patients, the volume receiving a dose above the threshold dose was 0.11 mL and 0.12 mL for the optic nerves and chiasm, respectively; the volume receiving a dose more than 105% of the threshold dose was 0.05 mL and 0.01 mL, respectively.41
Nervous System: Hearing
Organ Function and Clinical Significance
The cochlea and acoustic nerve are the essential auditory structures that are susceptible to radiation injury and consequential sensory neural hearing loss. These are small structures and, therefore, dose-volume measures are less determinable and clinically relevant. Other dose-dependent susceptible parts of the auditory system include the external ear and ear canal, tympanic membrane, ossicles, and eustachian tube.60 Platinum-based chemotherapy also is a well-established cause of sensory neural hearing loss. Factors such as baseline function and patient age are also relevant.
Dose-Volume Data
Several studies suggest that the dose to the cochlea correlates with the rate of sensory neural hearing loss. A study from the University of Florida showed that the incidence of sensory neural hearing loss increased consistently with the dose to the cochlea; the 10-year actuarial risk of sensory neural hearing loss was 3% at doses of less than 60.5 Gy versus 37% at doses of more than 60.5 Gy .60
Several other studies have shown hearing loss to be directly related to the inner-ear dose,61–65 with sensory neural hearing loss becoming more apparent at doses of more than 45 to 50 Gy.62,64,65 Cisplatin dose is also relevant to the threshold for auditory impairment. Cisplatin doses as low as 270 mg/m2 can result in hearing loss when combined with cranial radiotherapy dosages of 40 to 50 Gy.66 The sequence of chemoradiotherapy also influences risk. Risk and severity of ototoxicity are greater when cisplatin is administered after cranial irradiation.
Parotid Glands
Dose-Volume Data
The University of Michigan has published several studies investigating radiation dose-volume effects on serially measured stimulated and unstimulated salivary flow from a given parotid gland. With salivary flow measured up to 12 months after irradiation, significant parotid sparing was observed after a mean parotid dose below 24 Gy (for unstimulated flow) to 26 Gy (for stimulated flow).68,69,70 Mean doses correlated with a V15 of 67% or less, a V30 of 45% or less, and a V45 of 24% or less. The TD50 was 28.4 Gy.
Investigators at Washington University also examined whole salivary flow. Their technique differed from that of the University of Michigan researchers in that they measured flow from all glands, though they included only patients whose submandibular glands received more than 50 Gy in an attempt to minimize this confounding variable.71,72 Salivary flow was noted to be exponentially reduced by approximately 0.054/Gy of the mean parotid dose (i.e., e(−0.054* mean dose)), equating to a reduction to 25% of the pretreatment salivary flow with a mean dose of 25.8 Gy, essentially equivalent to the University of Michigan number.73 The mean dose model was more predictive of the risk of late effects than threshold dose levels of V5 to V70 as well as other models studied.
Other groups have corroborated the mean dose as a significant variable affecting salivary function,74–79 with a Belgian study suggesting a lower threshold mean dose of 22.5 Gy.80 A Dutch group demonstrated that the TD50 for stimulated salivary function (risk of <25% of pretreatment rates) improved with time, with a TD50 of 34 Gy at 6 weeks to 40 Gy at 6 months, 42 Gy at 12 months, and 46 Gy at 5 years.81,82 In a recent University of Michigan study, with flow rates measured in 142 patients up to 24 months after irradiation, the salivary flow rate was modeled as a function of time.83 With mean parotid doses of less than 25 Gy, the model predicted salivary function recovery to the pretreatment level of functioning at 12 months. For mean parotid doses of more than 30 Gy, stimulated saliva did not return to pretreatment functioning after 2 years.
The radiation dose to the submandibular glands may also affect salivary function. In a study from Helsinki University, the mean unstimulated salivary flow was 60% of the pretreatment function among patients who had one submandibular gland spared (mean dose of 26 Gy and range from 21 to 34 Gy) and 25% among those who did not (p = .006).84 However, sparing of a submandibular gland did not affect the stimulated saliva flow rates. Investigators from Utrecht have demonstrated that the mean submandibular dose is a significant variable affecting the sensation of sticky saliva.85
Larynx and Pharynx
Organ Function and Clinical Significance
The larynx and pharynx are involved with phonation and swallowing, respectively. Late complications include laryngeal edema and fibrosis, laryngeal dysfunction, dysphagia, and necrosis. A study from the University of Michigan showed that damage to the pharyngeal constrictors and the glottic and supraglottic larynx may cause dysphagia and aspiration after chemoradiation.87
Dose-Volume Data: Larynx
In a study from the University of Texas at Galveston (with most patients receiving irradiation alone), the mean laryngeal dose and laryngeal V30 to V70 were significantly associated with laryngeal edema of grade 2 or higher with a univariate analysis, whereas the mean laryngeal dose and N stage were significant with multivariate analysis.88 The V50, which was highly correlated with the mean laryngeal dose, was significant in a multivariate analysis in which the mean laryngeal dose was replaced by V50. The 1-year rate of grade 2 or higher edema was 20% after a mean laryngeal dose of 43.5 Gy (or V50 <27%), versus 45% after a mean dose of 44 to 57 Gy (or 94% < V50 > 27%) versus more than 80% after a mean dose of more than 57 Gy (or V50 >94%).
There is a paucity of data correlating dose-volume metrics with vocal dysfunction. Generally, after therapeutic doses of 60 to 66 Gy for early-stage glottic cancer, the risks of vocal dysfunction are low. In a study from the University of Iowa, point doses in excess of 66 Gy to the aryepiglottic folds, preepiglottic space, false vocal cords, and lateral pharyngeal walls resulted in a sharp increase in the risk of vocal dysfunction.89
Dose-Volume Data: Swallowing
Several studies have investigated dose-volume metrics predictive of swallowing dysfunction. In a study from the University of Michigan, the mean dose to the pharyngeal constrictors was correlated to the risk of aspiration.91 The risk of aspiration increased with a mean dose of more than 60 Gy to the pharyngeal constrictors, and with a V40 of more than 90%, V50 of more than 80%, V60 of more than 70%, and V65 of more than 50%, and with a V50 of more than 50% for the larynx. Three patients who developed strictures had a V70 of the pharyngeal constrictor of more than 50%.
In a study from Aarhus University, several significant correlations were found between both subjective and objective swallowing problems and DVH parameters of the base of the tongue, pharyngeal constrictors, supraglottic larynx, esophageal sphincter, and glottic larynx.92 Doses of less than 60 Gy to the supraglottic region, larynx, and upper esophageal sphincter resulted in a low risk of swallowing difficulties and aspiration.
In a study from the University of Iowa, point doses to the false vocal cords, lateral pharyngeal walls, and upper esophageal sphincter were correlated with dietary changes.89 As an example, the dose to the left lower pharyngeal wall for patients who had not had oral intake 1 year after treatment was 79.7 Gy versus 65.1 Gy for those with an unrestricted diet. A greater radiation dose to the aryepiglottic folds was associated with greater weight loss, and a greater radiation dose to the false vocal cords was associated with percutaneous endoscopic gastrostomy (PEG) tube use.
In a study from Rotterdam, doses of more than 50 Gy to the pharyngeal constrictors resulted in a 20% probability of dysphagia, with an incremental 19% risk for each additional 10 Gy to the constrictors.93 A study from the Dana-Farber Cancer Institute94 also demonstrated that doses to the pharyngeal constrictors of 50 Gy or more, as well as doses to the larynx of 50 Gy or more, were significantly associated with aspiration and stricture risk.
Lungs
Organ Function and Clinical Significance
Radiation damage to the lung can result in pneumonitis and fibrosis. Symptomatic radiation pneumonitis is characterized by dyspnea, cough, and sometimes a low-grade fever, typically occurring several weeks to months after irradiation. Long-term lung fibrosis can lead to respiratory insufficiency. It is often challenging to distinguish radiation-related pulmonary symptoms from comorbid illnesses (e.g., exacerbation of chronic obstructive pulmonary disease [COPD], infection, or cardiac events).95 Objective reductions in the lung’s ability to move and exchange gas can be measured by formal pulmonary function tests (PFTs).
Dose-Volume Data: Pneumonitis and Fibrosis
Several parameters have been shown to be associated with the risk of radiation pneumonitis, including the V5 to V70, mean lung dose (MLD), and model-based parameters.96,97 These variables are correlated with each other, accounting for the fact that in most studies examining a range of Vx variables, many or most are significant.* Table 13-2 summarizes many of the studies discussed below.
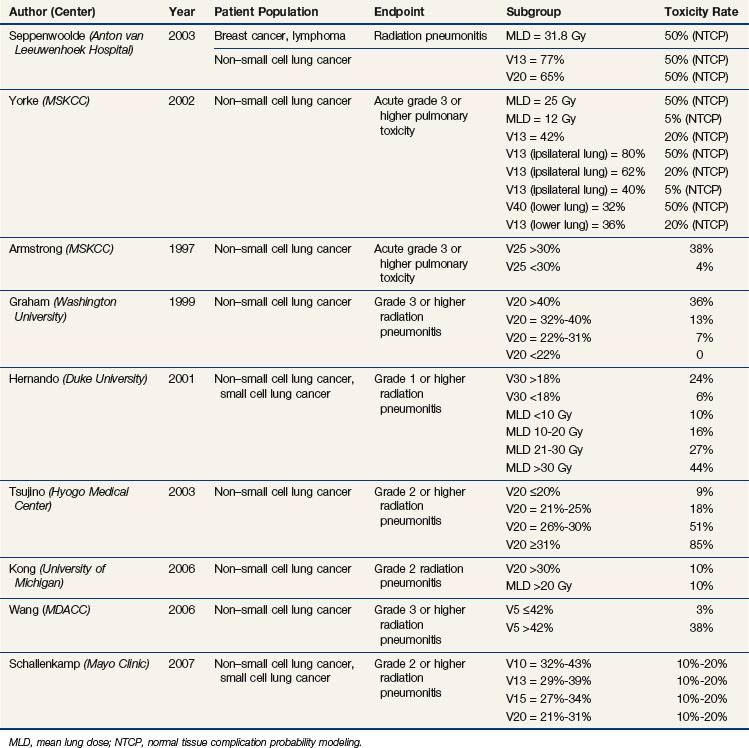
A normal tissue complication probability (NTCP) analysis from the Netherlands, in collaboration with the University of Michigan, suggests that using the mean lung dose (linear function) is more predictive than using the Vx (step function).101 However, the V13 tended to be more predictive in situations where the mean lung dose exceeded 20 Gy or the V13 exceeded 50%. The TD50 values in this study were a mean lung dose of 30.8 Gy, V13 of more than 77%, and V20 of more than 65%, similar to the mean lung dose of 31.8 Gy reported in an earlier multiinstitutional study.112 From an NTCP analysis from the Memorial Sloan-Kettering Cancer Center (MSKCC),99 a mean lung dose of approximately 26 Gy, a V13 of more than 80% of the ipsilateral lung, or a V40 of more than 32% of the lower lung resulted in a 50% risk of developing late complications. A mean lung dose of approximately 12 Gy or a V13 of more than 40% of the ipsilateral lung resulted in a 5% late complication risk. A V13 of 36% of the lower lung, 42% of the total lung, or 62% of the ipsilateral lung resulted in a 20% risk of developing late grade 3 or higher complications.
In a 1997 study from the MSKCC, of patients treated with irradiation alone, there was a significantly increased risk of grade 3 or higher pulmonary toxicity, 38% with a V25 of more than 30% versus 4% with a V25 of less than 30% (p = .04).113 In subsequent studies from this same group, significant variables for predicting grade 3 or higher pulmonary toxicity included the mean lung dose, the range of V5 to V40 of the total lung, V5 to V40 of the ipsilateral lung, and V5 to V50 of the lower lung.99,104 The range of V5 to V20 for the ipsilateral lung was most predictive.
Washington University investigators also demonstrated that the risk of pneumonitis significantly correlated with the V20; the 2-year incidence of grade 2 or higher radiation injury was 36% versus 13% versus 7% versus 0%, with a V20 of more than 40%, 32% to 40%, 22% to 31%, and less than 22% (p = .0013), respectively.96 In another study from Washington University, radiation pneumonitis was significantly correlated with the V5 to V80, with peak significance in the ranges of V5 to V15 and V70 to V75; radiation pneumonitis was also significantly correlated with the dose delivered to 5% to 100% of the lung (D5 to D100), with peak significance in the D30 to D40 and V90 to V95 ranges.107
In a 2001 study from Duke University (in which 18% of patients received concurrent chemoradiotherapy), a V30 of more than 18% versus less than 18% was associated with a risk of grade 1 or higher radiation pneumonitis of 24% versus 6% (p = .0003).98 Mean lung doses of less than 10 Gy, 10 to 20 Gy, 21 to 30 Gy, and more than 30 Gy were associated with risks of 10%, 16%, 27%, and 44%, respectively. A Japanese study of patients treated with platinum-based chemoradiotherapy found a 6-month risk of grade 2 or higher radiation pneumonitis to be 85%, 51%, 18.3%, and 8.7% (p <.0001), with a V20 of 31% or higher, 26% to 30%, 21% to 25%, and 20% or less, respectively.114 In a University of Michigan study, a 10% risk for grade 2 or higher pneumonitis and fibrosis was associated with a V20 of more than 30% and a mean lung dose of more than 20 Gy. These thresholds provided a positive predictive value of 50% to 71% and a negative predictive value of 85% to 89%.115 In a study from the MDACC, the mean lung dose and V5 to −V65 were highly correlated with the risk of pneumonitis, and the V5 was the most significant factor in a multivariate analysis.106 For a V5 of 42% or less versus more than 42%, the risk of grade 3 or higher pneumonitis at 1 year was 3% versus 38% (p = .001). In a Mayo Clinic study, the V10 to V13 was most predictive of radiation pneumonitis; a V10 of 32% to 43%, V13 of 29% to 39%, V15 of 27% to 34%, and V20 of 21% to 31% resulted in a 10% to 20% risk of pneumonitis.111
Several dose escalation studies have used the V20, Veff, and/or NTCP (normal tissue complication probability) to allocate patients into given dose levels.116–119 In the RTOG 93-11 dose escalation study, patients with a V20 of less than 25% experienced a 7% to 16% 18-month actuarial rate of grade 3 or higher late lung toxicity with prescribed doses of 70.9 to 90.3 Gy; the absolute risk of grade 2 or higher late lung toxicity was 30% to 45%, with one fatal lung complication at the 90.3-Gy dose level. Patients with a V20 of 25% to 36% treated to doses of 70.9 to 77.4 Gy experienced 15% grade 3 or higher late toxicity at 18 months and an absolute risk of grade 2 or higher late lung toxicity of 40% to 60%.116 The D15 was the most predictive variable for radiation pneumonitis.110
In a Dutch study, the effect of regional dose in the lung was investigated, with the lung divided into central and peripheral, ipsilateral and contralateral, caudal and cranial, and anterior and posterior subvolumes.120 The mean regional dose to the posterior, caudal, ipsilateral, central, and peripheral lung subvolumes significantly correlated with the incidence of steroid-requiring radiation pneumonitis. In a similar study from the MSKCC, the risk of radiation pneumonitis was better correlated with the radiation dose to the inferior aspect of the lung rather than the superior aspect.99
Tumor location within the chest may also be a factor affecting risk of pneumonitis. In the above-mentioned study from Washington University,107 inferior tumor location was the most significant predictor of radiation pneumonitis. Tumor location was not a strong correlate to radiation pneumonitis in a study of patients treated in RTOG 93-11, perhaps attributable, in part, to differences in treatment (with RTOG 93-11 designed to treat smaller volumes to higher doses) and differences in tumor size and location (the RTOG 93-11 tumors tended to be smaller and more superiorly located).110 Using a combined data set of patients from RTOG 93-11 and Washington University, tumor location, in addition to mean lung dose, was significant.
IMRT has been demonstrated to provide unique dose distributions for some patients with advanced-stage non–small cell lung cancer.121 The IMRT-based dose distributions appear to reduce the risk of normal tissue injury in patients with non–small cell lung cancer. Investigators at the MDACC compared their rates of lung toxicity in patients treated with IMRT versus three-dimensional planning and noted a reduction in toxicity with the IMRT approach.122 Investigators at the MSKCC noted a similarly low rate of clinical lung injury in patients with non–small cell cancer treated with IMRT.123 In the MDACC study, a V5 of more than 70% was associated with a 21% risk of grade 3 or higher pneumonitis versus a 2% risk with a V5 of 70% or less (p = .017).
IMRT has also been used to treat patients with mesothelioma. In a study from the Dana-Farber Cancer Institute, in which patients received thoracic IMRT after pneumonectomy for mesothelioma, 6 of 13 patients developed fatal pneumonitis.124 The median V20, V5, and mean lung dose for patients who developed pneumonitis was 17.6%, 98.6%, and 15.2 Gy, respectively, versus 10.9%, 90%, and 12.9 Gy for those who did not develop pneumonitis. Although these differences were not significant, the severity of the toxicities merits caution when large volumes are being treated after a pneumonectomy. In a study from Duke University, 1 of 13 patients treated with IMRT for mesothelioma died from pneumonitis, and 2 others developed symptomatic pneumonitis.125



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


