Sarcomatoid (Sarcomatous) Carcinoma
Sanja Dacic
Sarcomatoid carcinomas are rare and make up only 0.3% to 1.3% of all lung malignancies.1 These tumors are defined by 2004 WHO criteria as a poorly differentiated non-small cell lung carcinomas (NCSLCs) that contain a component of sarcoma or sarcoma-like (spindle or giant cells or both) differentiation. Although the diagnosis may be suspected on transbronchial biopsy or fine needle aspiration, surgical resection is necessary for definitive classification and diagnosis.
SARCOMATOID CARCINOMA, CYTOLOGY
Cytologically, sarcomatoid carcinomas exhibit spindle cell elements. Malignant epithelial, giant cell, or heterologous (e.g., malignant cartilaginous, osseous, or rhabdomyomatous) elements may be present as well (Fig. 13-1).
SARCOMATOID CARCINOMA, GROSS FEATURES
Sarcomatoid carcinomas can arise in the central or peripheral lung, usually as a large mass between 3 and 11 cm. Grossly, the cut surface is gray-white with areas of necrosis and hemorrhage (Fig. 13-2).
SARCOMATOID CARCINOMA, HISTOLOGY
Five subgroups of sarcomatoid carcinomas are recognized including pleomorphic carcinomas, spindle cell carcinomas, giant cell carcinoma, carcinosarcoma, and pulmonary blastoma. Three of these entities are discussed below. Giant cell carcinoma and pulmonary blastoma are discussed separately in Chapters 14 and 15.
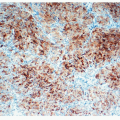
Pleomorphic carcinoma consists of a poorly differentiated squamous cell carcinoma, adenocarcinoma, or large cell carcinoma admixed with spindle or giant cells constituting >10% of the tumor (Fig. 13-3). Spindle cells may have epithelioid or mesenchymal appearance. The stroma may be fibrous or myxoid. Malignant giant cells are polygonal, are uninucleated or multinucleated, and have dense eosinophilic cytoplasm and pleomorphic nuclei. Emperiopolesis is common (Fig. 13-4). Large vessel invasion associated with necrosis is usually present.2,3,4,5 and 6
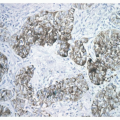
Carcinosarcoma is a malignant tumor consisting of a mixture of carcinoma and sarcoma containing differentiated sarcomatous elements, such as malignant cartilage, bone, or skeletal muscle (Fig. 13-5). Squamous cell carcinoma is the most common carcinomatous component (45%-70%), followed by adenocarcinoma (20%—31%) and large cell carcinoma (10%). An undifferentiated spindle cell sarcoma component is most frequently present, followed by rhabdomyosarcoma, osteosarcoma, or chondrosarcoma. More than one differentiated sarcomatous component may be present. Sarcomatous component is often the predominant component, and the foci of carcinoma are often small.7,8
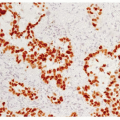
Spindle cell carcinoma is defined as an NSCLC consisting of only spindle-shaped tumor cells which are identical to the spindle cell component of pleomorphic carcinomas (Fig. 13-6).
Irregular fascicles of obviously malignant spindle cells with nuclear hyperchromasia and prominent nucleoli are seen. Adenocarcinoma, giant cell, squamous cell, or large cell carcinoma are not seen.5,8,9
Irregular fascicles of obviously malignant spindle cells with nuclear hyperchromasia and prominent nucleoli are seen. Adenocarcinoma, giant cell, squamous cell, or large cell carcinoma are not seen.5,8,9
 FIGURE 13-1 High-power image of Papstained cytology preparation of sarcomatoid carcinoma showing an enlarged, hyperchromatic malignant spindle tumor cell within a background of bronchial mucosal cells. |
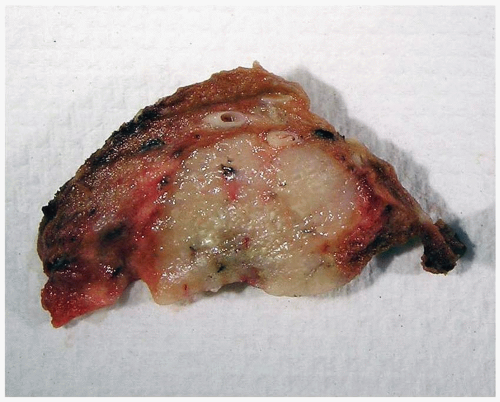 FIGURE 13-2 Gross image of a wedge resection specimen containing sarcomatoid carcinoma, specifically in this case chondrosarcoma, showing a peripheral well-circumscribed tumor with a glistening, off-white cut surface and focal small areas of hemorrhage. |
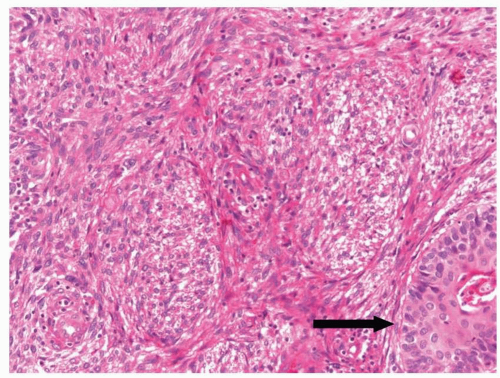 FIGURE 13-3 Medium-power image of pleomorphic carcinoma composed of a conventional squamous cell carcinoma (arrow) admixed with more than 10% of malignant spindle cells. |
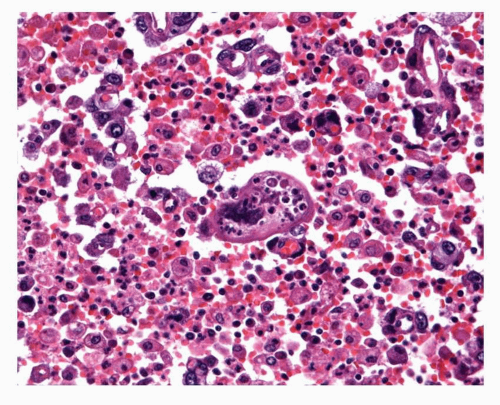 FIGURE 13-4 High-power image of sarcomatoid carcinoma exhibiting emperiopolesis. |
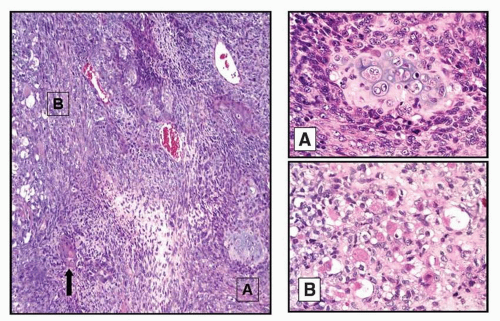 FIGURE 13-5 Medium-power image of carcinosarcoma exhibiting a mixture of a conventional squamous cell carcinoma (arrow) as well as true sarcomatous components including chondrosarcoma (A) and rhabdomyosarcoma (B).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|