I.C.001 Abetalipoproteinemia
I.C.001
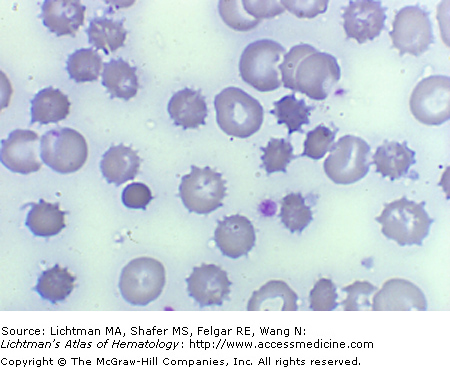
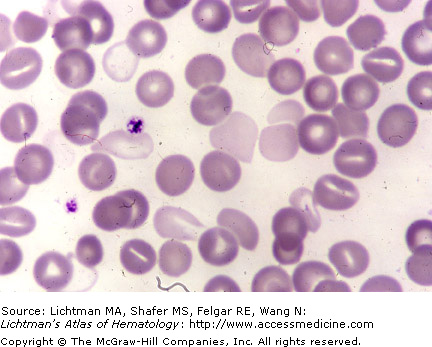
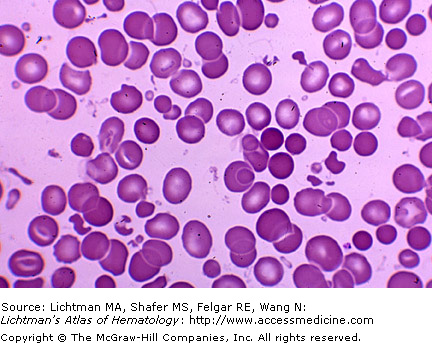
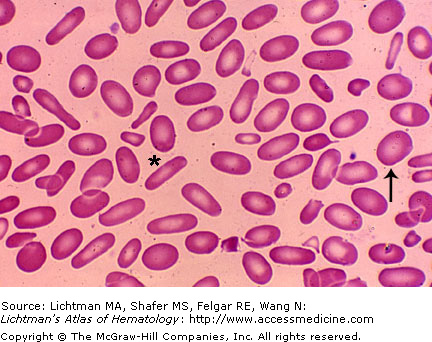
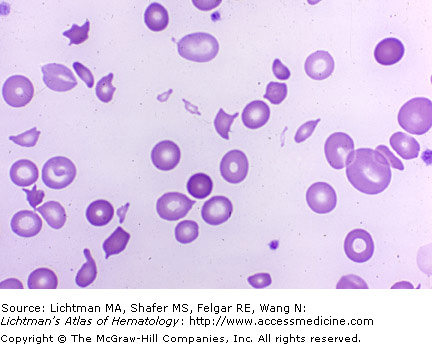
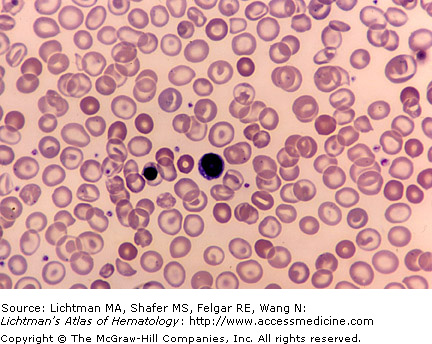
Abetalipoproteinemia. Blood film. Patients with this inherited absence of products of the apolipoprotein B gene characteristically have over 50% acanthocytes, red cells with irregular, sharp projections, in the blood. The red cell membrane abnormality is thought to reflect an excess of sphingomyelin in the outer leaflet of the membrane lipid bilayer, leading to excess surface area and sharp, irregular, spike like folds in the red cell surface. Erythroblasts do not display the abnormality and circulating cells develop it as they age in the circulation.
I.C.002 Abetalipoproteinemia. Acanthocytes
I.C.002
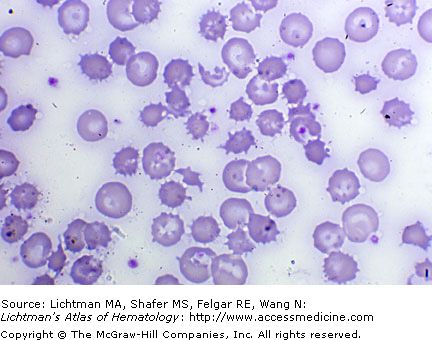
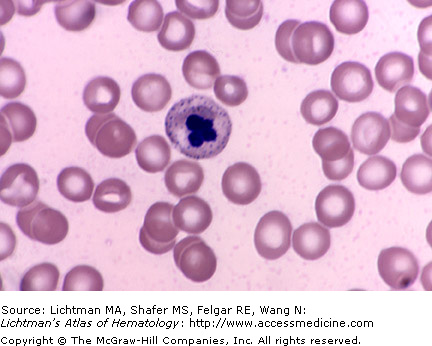
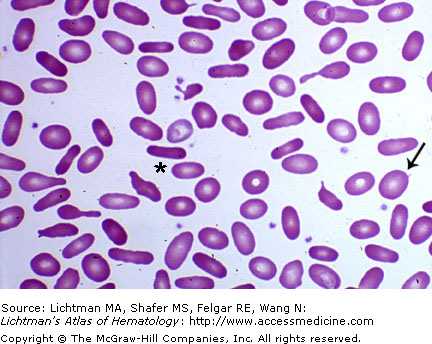
Acanthocytosis. Abetalipoproteinemia. Blood film. Patients with this inherited absence of products of the apolipoprotein B gene characteristically have over 50% acanthocytes, red cells with irregular sharp projections, in the blood. The red cell membrane abnormality is thought to reflect an excess of sphingomyelin in the outer leaflet of the membrane lipid bilayer, leading to excess surface area and sharp spike like folds in the red cell surface. Erythroblasts do not display the abnormality and circulating cells develop it as they age in the circulation.
I.C.003 Acanthocytes. Spur Cell Anemia

I.C.003
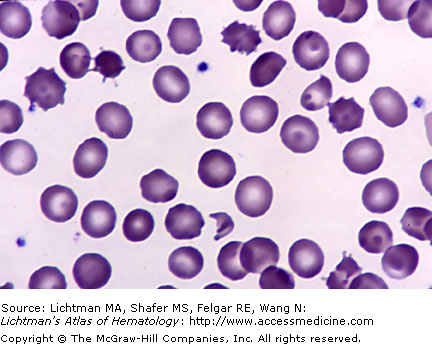
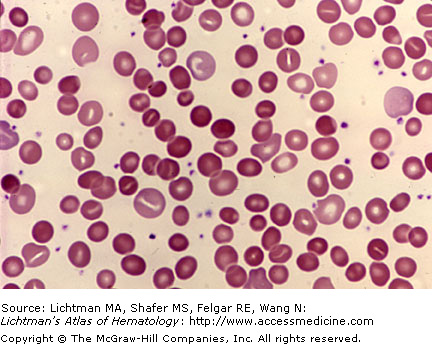
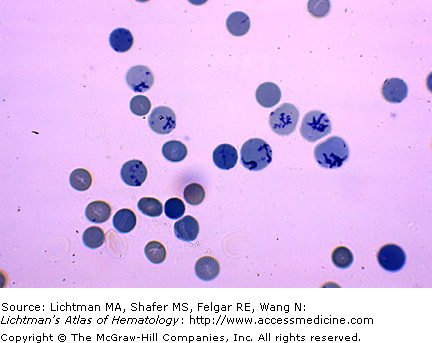
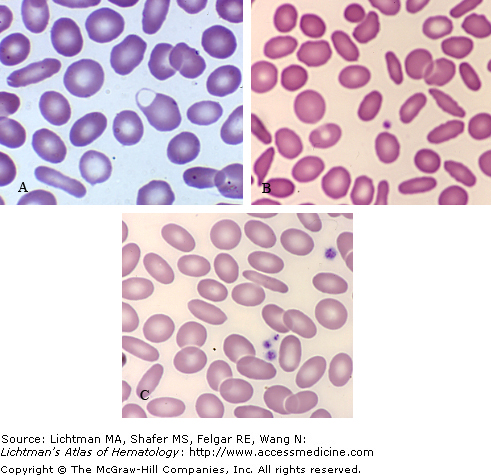
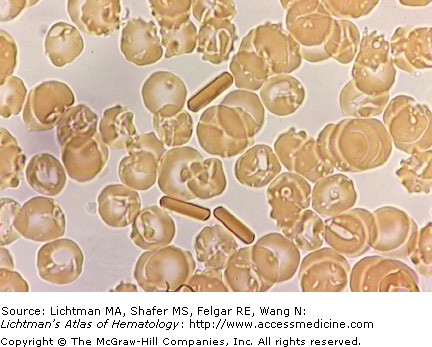
Acanthocytosis. Blood film. Spur cell anemia. Acanthocytes are red cells, often contracted in size and hyperchromatic, with irregularly placed, short, pointed projections from the cell surface. They are characteristic of patients with abetalipoproteinemia and may be seen in smaller numbers in a variety of metabolic disorders, such as severe chronic liver or renal disease, in the post-splenectomy state, and in small numbers in a variety of blood cell disorders affecting red cells. This case is an example of spur cell anemia in chronic severe liver disease. Note spherocytes, stomatocytes, and many spheroacanthocytes, the latter are small dense, speculated cells.
I.C.004 Alloimmune Hemolytic Anemia, ABO Incompatibility
I.C.004
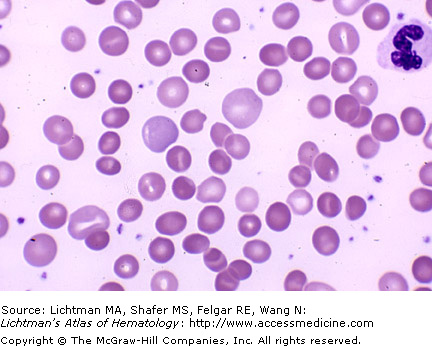
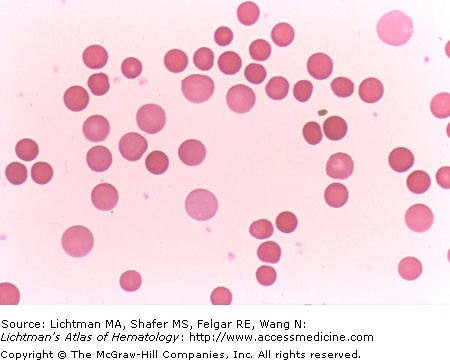
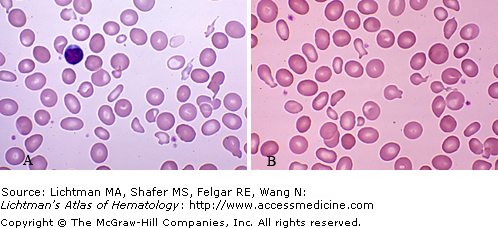
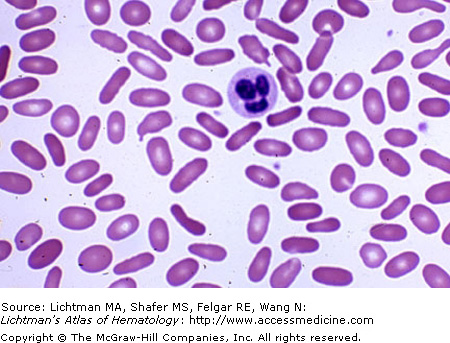
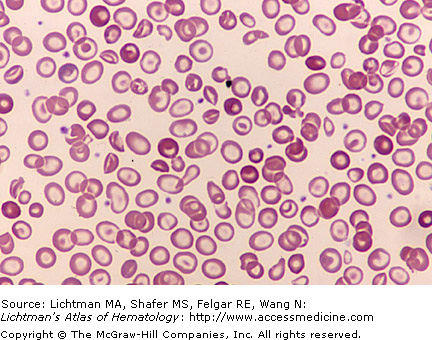
Alloimmune hemolytic anemia, ABO incompatibility. Blood film. Note the polychromatophilic macrocytes (reticulocytes) and spherocytes, characteristics of a severe spherocytic hemolytic anemia. Nucleated red cells, a striking feature of Rh-mediated alloimmune hemolytic anemia are less prominent in ABO maternal-fetal incompatibility.
I.C.005 Alloimmune Hemolytic Anemia, Rh Incompatibility

I.C.005
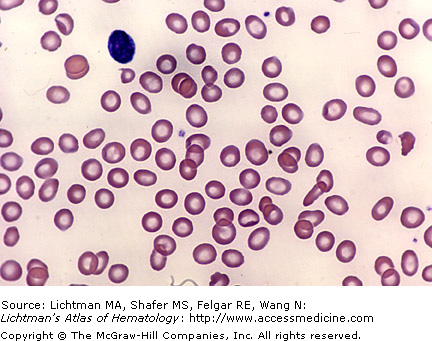
Alloimmune hemolytic anemia, Rh incompatibility. Blood film. Note the polychromatophilic macrocytes (reticulocytes), the nucleated red cells, and the ejected erythroblast nuclei. Spherocytes are present. The intense erythroblastosis (nucleated red cells in the blood) is characteristic of Rh-mediated alloimmune hemolysis.
I.C.006 Anorexia Nervosa
I.C.007 Anorexia Nervosa

I.C.008 Arsenic Hydride (Arsine Gas) Poisoning
I.C.008
Arsenic hydride (arsine gas) poisoning. Blood film. Arsine is a gas formed when metals or ores containing arsenic are exposed to acid. Workers soldering, etching, galvanizing, and lead plating are at risk. This highly toxic gas when inhaled can cause multiorgan injury. The red cells are rapidly hemolyzed as a result of membrane injury. Signs of intravascular hemolysis quickly ensue. The red cells lose hemoglobin and circulating ghost cells may be present. Changes related to oxidant injury may also be present (irregular forms, bitten cells). In this film several red cells are nearly ghosts with very light staining resulting from leakage of hemoglobin through pores in damaged membranes.
I.C.009 Arsenic Poisoning
I.C.009
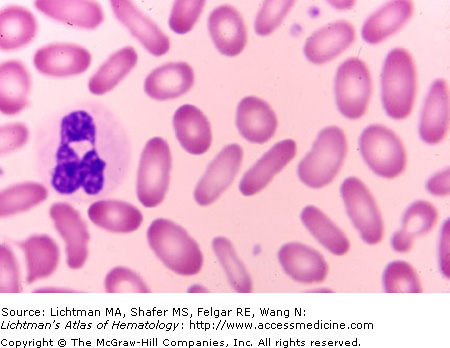
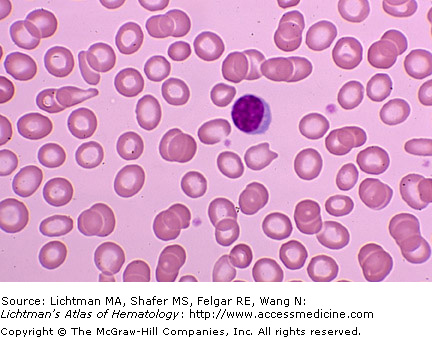
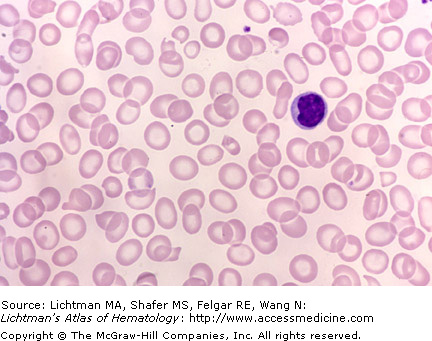
Arsenic poisoning. Blood film. The red cells show mild hypochromia and anisocytosis. The nucleated red cell in the blood shows a marked abnormality of the nucleus (lobulation) and intense stippling. This reflected the dyserythropoietic features of the erythroblasts in marrow in this disorder.
I.C.010 Arsenic Poisoning

I.C.011 Asplenia, Congenital

I.C.012 Autoimmune Hemolytic Anemia, Warm Antibody Type
I.C.013 Autoimmune Hemolytic Anemia, Warm Antibody Type

I.C.014 Autoimmune Hemolytic Anemia, Warm Antibody Type
I.C.015 Autoimmune Hemolytic Anemia, Warm Antibody Type
I.C.016 Autoimmune Hemolytic Anemia, Warm Antibody Type

I.C.017 Autoimmune Hemolytic Anemia, Warm Antibody Type
I.C.017
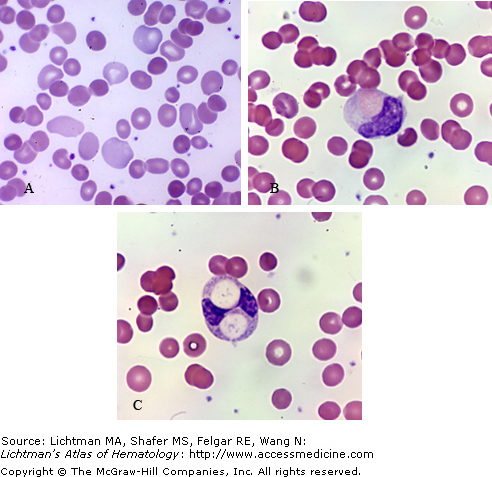
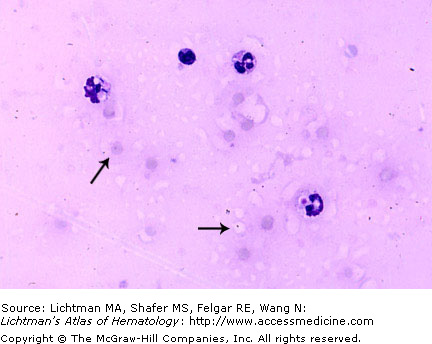
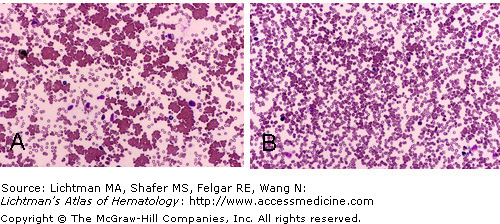
Autoimmune Hemolytic Anemia. Blood films. (A) Classical appearance of autoimmune hemolytic anemia with numerous microspherocytes, many without a pale center because of severe spheroidicity. Note hyperchromatic coloration of spheres, a reflection of an increased mean cell hemoglobin concentration and absence of a central concavity. In the disc to sphere transformation, there is a decrease in the surface/volume ratio. Note the polychromatophilic macrocytes representing reticulocytes, the reflection of the normal erythropoietic response to hemolysis. (B and C) Two cases of autoimmune hemolytic anemia in which erythrophagocytosis of antibody-coated erythrocytes by monocytes is evident. Note spherocytic red cells in blood film. Note in (C) two red cell circular remnants evident.
I.C.018 Autoimmune Hemolytic Anemia, Post-Splenectomy
I.C.018
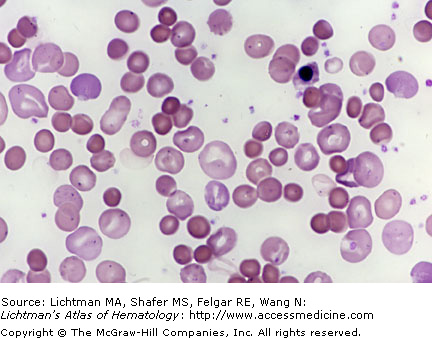
Autoimmune hemolytic anemia, post-splenectomy. Blood film. Unsuccessful splenectomy. Persistent extreme spherocytosis and massive increase in polychromatophilic macrocytes (reticulocytes). Note many large, bluish, cells many with folds of redundant membrane. Stress reticulocytes have a higher surface area to volume ratio. Nucleated red cell also evident.
I.C.019 Burns, Moderately Severe

I.C.020 Burns, Moderately Severe Changes
I.C.021 Burns, Severe Changes

I.C.022 Burns, Severe Changes
I.C.023 Clostridium Perfringens Exotoxin Hemolytic Anemia
I.C.023
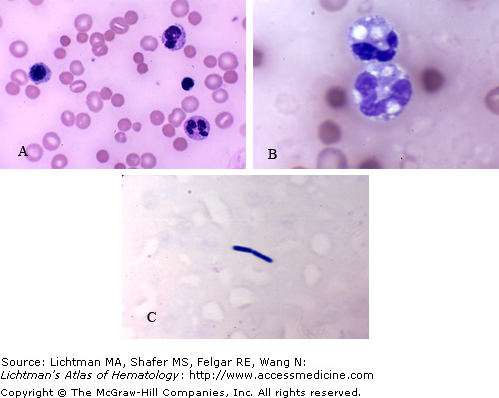
Clostridium Perfringens exotoxin hemolytic anemia. Blood films. (A) Frequent microspherocytes admixed with transfused cells. Spherocytosis results from the effect of the Clostridial alpha-exotoxin, a lecithinase, on the lipoproteins of the red cell membrane. The effect leads to the release of lysolecithins, potent hemolytic agents. (B) Vacuolated neutrophils reflecting erythrophagocytosis and erythrocyte intracellular lysis and-or the ingestion of Clostridial organisms. (C) Clostridium perfringens in blood film.
I.C.024 Clostridium Perfringens Sepsis

I.C.024
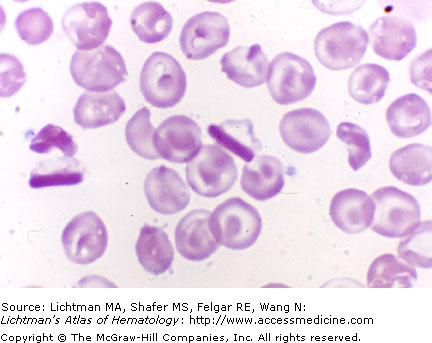
Clostridium perfringens sepsis. Blood film. Intense spherocytosis from the direct effect of the clostridial alpha-exotoxin, a lecithinase, on the lipoproteins in the red cell membrane. The effect leads to release of lysolecithins, potent hemolytic agents. Proteolysis may also participate in the damage to the red cell membrane. The thin red cell layer in the blood film is a reflection of the profound anemia, resulting from rapid hemolysis. Polychromatophilic macrocytes (reticulocytes) are present, also.
I.C.025 Clostridium Perfringens Sepsis
I.C.026 Cold Hemagglutinin Disease
I.C.026
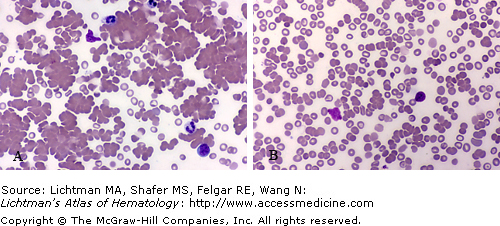
Cold Hemagglutinin Disease. (A) Blood at room temperature. Not striking agglutination. (B) Blood warmed to 37oC. Absence of agglutination. The temperature difference between non-agglutination and agglutination is referred to as the thermal amplitude. This difference is related in part to the titer of cold agglutinins in cold hemagglutinin disease. In general, the higher the titer of cold agglutinins the higher the temperature at which agglutination may occur. The temperature in the surface vessels of some acral parts permits agglutination in the circulation in those areas.
I.C.027 Cold Hemagglutinin Disease
I.C.027
Cold hemagglutinin disease. Blood films. (A) Marked red cell agglutination at room temperature. (B) Decreased red cell agglutination with blood and glass slide maintained at 37oC. Cold agglutinins are nearly always plasma IgM immunoglobulins. The thermal amplitude of the protein (temperature at which its agglutinating capacity is absent) determines the clinical severity of its effects on small vessel blood flow in superficial vessels (e.g., digits, ear lobes).
I.C.028 Congenital Dyserythropoietic Anemia
I.C.028
Congenital Dyserythropoietic Anemia. Blood Films. (A) Type I and (B) Type II. Note anisocytosis with some microcytes and occasional macrocytes. Slight anisochromia with some hypochromic cells normocytic and poikilocytic cells. Marked poikilocytosis with elliptocytes, tear-drop cells, fragments of red cells, and occasional spherocytes. The Atlas section on Marrow has several examples of marrow dyserythropoiesis in these disorders.
I.C.029 Congenital Dyserythropoietic Anemia
I.C.030 Disseminated Intravascular Coagulation
I.C.031 Disseminated Intravascular Coagulation

I.C.032 Elliptocytes, Hereditary
I.C.033 Elliptocytosis, Hereditary
I.C.034 Elliptocytosis, Hereditary

I.C.035 Elliptocytosis, Hereditary

I.C.035
Elliptocytosis, Hereditary. (A–C) Blood films. Note the variation among three different patient’s blood films in the red cell shape. (A) Higher ovalocyte to elliptocyte ratio than (B) or (C). (B) Frequent very small poikiolocytes, many with roughly elliptical dimensions, unlike (A) or (C). (C) Occasional elliptocytes with long tails.
I.C.036 Elliptocytosis, Hereditary
I.C.037 Elliptocytosis, Hereditary
I.C.038 Elliptocytosis, Hereditary
I.C.038
Hereditary elliptocytosis. Blood film. Note approximately equal prevalence of elliptical-shaped (cigar-shaped) red cells and of oval-shaped (football-shaped) red cells. The proportion of elliptocytes and ovalocytes vary among patients with the hereditary elliptocytosis gene. Some patients have almost entirely elliptical shaped red cells and others have nearly all ovalocytes with any type of mixture in between. Some use the convention of considering either oval or elliptical cells elliptocytes with the designation types I, II, or III depending on the degree of elliptocytosis.
I.C.039 Fava Bean-Induced Hemolysis
I.C.039
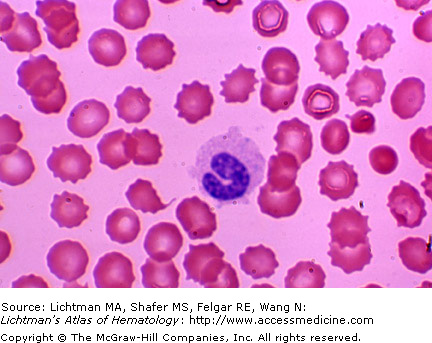
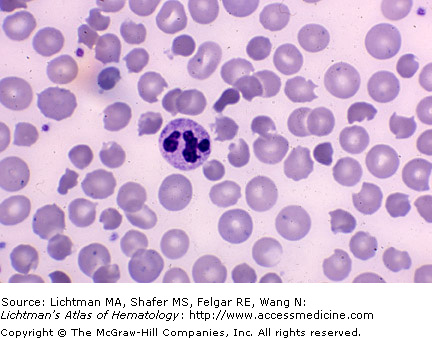
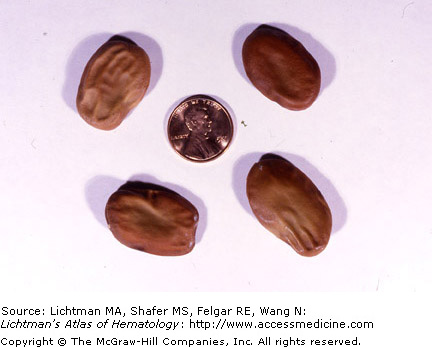
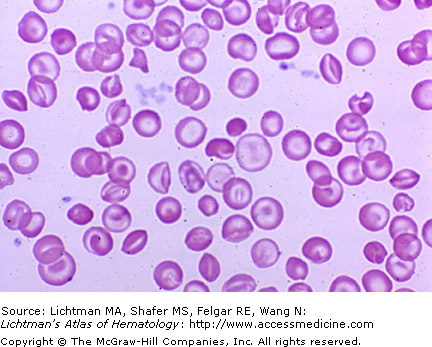
Fava bean-induced hemolysis. Blood film. Anisocytosis resulting from presence of polychromatophilic macrocytes (reticulocytes) and smaller poikilocytes. Characteristic keratocytes (bitten or helmet cells) are present reflecting oxidant-induced hemolysis. Spherocytes or keratospherocytes are present.
I.C.041 Fragmentation Hemolytic Anemia
I.C.041
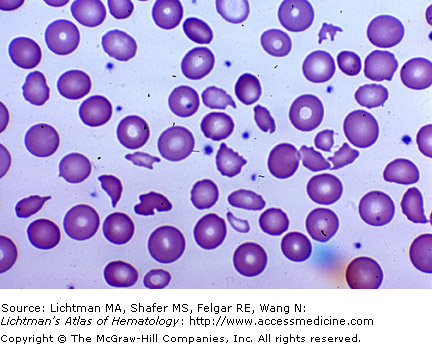
Fragmentation hemolytic anemia. Blood film. Poorly seated synthetic heart valves can result in sufficient shearing forces in blood ejected from the ventricle to fracture red cells. Note small misshapen red cell fragments. This problem has been largely resolved by use of valves that do not injure red cells significantly.
I.C.042 Fragmentation Hemolytic Anemia
I.C.043 Glucose-6-Phosphate Dehydrogenase Deficiency
I.C.043
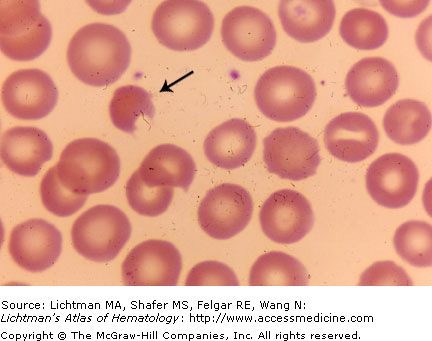
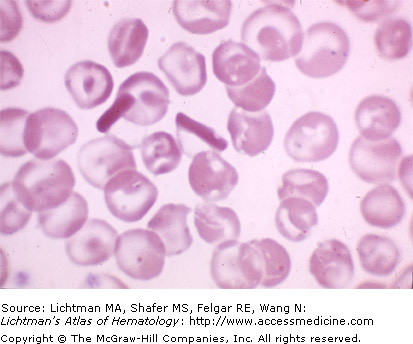
Glucose-6-phosphate dehydrogenase deficiency. Blood film. The arrow points to a keratocyte or “bite” cell, characteristic of hemolytic disease induced by oxidative stress in patients with this red cell enzyme deficiency. The deformity is thought to be the result of oxidative damage that leaves a segment of the cell appearing as if a bite was taken out of it.
I.C.044 Glucose-6-Phosphate Dehydrogenase Deficiency

I.C.044
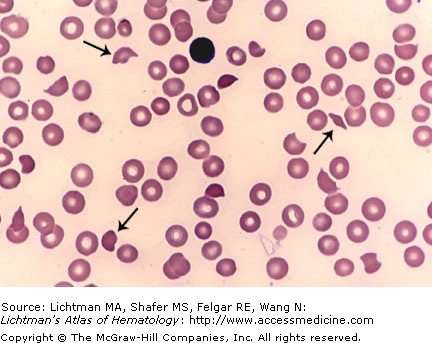
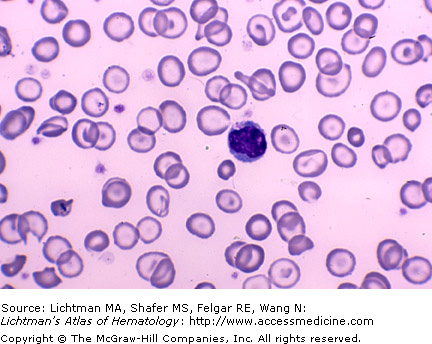
Glucose-6-phosphate dehydrogenase deficiency. Blood film. The two arrows points to keratocytes or “bite” cell, characteristic of hemolytic disease induced by oxidative stress in patients with this red cell enzyme deficiency. The deformity is thought to be the result of oxidative damage that leaves a segment of the cell appearing as if a bite was taken out of it. There are eight such cells in this field.
I.C.045 Hemoglobin CC Disease

I.C.046 Hemoglobin CC Disease
I.C.047 Hemoglobin CC Disease. Phase Contrast Micrograph
I.C.047
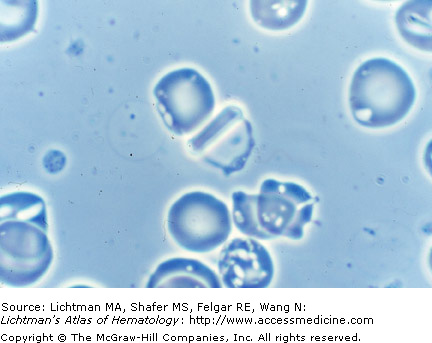
Hemoglobin CC disease. Phase contrast micrograph. Post-splenectomy. Note elliptical crystal-like precipitate in cell in center of field. Target cells are not evident in a wet preparation of Hemoglobin CC red cells. Their increased resistance to osmotic lysis, however, supports an increased surface area to volume ratio.
I.C.048 Hemoglobin CC Disease
I.C.049 Hemoglobin C and Beta Thalassemia Trait
I.C.049
Hemoglobin C and beta thalassemia trait. Blood film. In this combined hemoglobinopathy, the effect of C hemoglobin inducing target cells dominates the blood picture. Occasional dense spherocytes are also present, characteristic of the effect of C hemoglobin. Occasional poikilocytes, microcytes, and hypochromic cells may reflect the contribution of thalassemia to the red cell changes.
I.C.050 Hemoglobin C and Beta Thalassemia Trait
I.C.051 Hemoglobin DD Disease

I.C.052 Hemoglobin EE Disease

I.C.053 Hemoglobin EE Disease and Iron Deficiency
I.C.054 Hemoglobin E Trait
I.C.055 Hemoglobin E and alpha-thalassemia trait
I.C.056 Hemoglobin E and homozygous alpha-thalassemia

I.C.057 Hemoglobin F, Hereditary Persistence

I.C.057
Hemoglobin F, Hereditary Persistence. (A) Low power. (B) Higher power. Images of an acid elution of blood cells. Hemoglobin A is eluted under acidic conditions, whereas hemoglobin F is not. The more densely reddish-colored red cells represent residual hemoglobin F containing cells after acid elution. Normally, such cells are uncommon, less than 1% of red cells. The frequency of F-containing red cells may be as high as 100% in homozygotes for hereditary persistence of F hemoglobin (HPFH) and is usually between 10 and 40% in heterozygotes. It is an innocuous condition. In most cases, HPFH results from either a large deletion in the beta globin gene cluster or by point mutations in the gamma globin genes (HBG1 or HBG2).
I.C.058 Hemoglobin F, Hereditary Persistence

I.C.058
Hemoglobin F, hereditary persistence. Kleinhaver-Betke preparation for F hemoglobin. The reddish stained cells have increased F hemoglobin content. Usually in this disorder about 50% or more of cells react with this stain. F hemoglobin containing cells can also be analyzed by an antibody method.
I.C.059 Hemoglobin H Disease
I.C.060 Hemoglobin H Disease
I.C.061 Hemoglobin H Disease. Phase Contrast Micrograph

I.C.062 Hemoglobin H Disease
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


