Radiologic Imaging Concerns
Jeffrey A. Bennett
The oropharynx provides a challenge to imaging because of its abundant lymphoid tissue, which normally enhances and has variable thickness. Small superficial mucosal tumors may not be seen on CT or MRI for this reason. Indeed, small lesions may not be seen with direct visualization if they are hiding within deep crypts in the lymphatic tissue. Therefore, tumor can only be reliably identified on imaging studies if it infiltrates into the deep soft tissue planes (Fig. 17-15). An additional challenge to CT imaging is streak artifact from dental hardware, which may necessitate changing the gantry angle to achieve adequate visualization of the entire oropharynx. Tongue motion and swallowing will degrade the images as well, which is certainly a problem for MRI, but is less of a problem with high-speed multidetector CT scanning. Suggested protocols are given in Figures 17-16 and 17-17.
Even though the superficial mucosal extent of a tumor may not be well seen with CT or MRI, both imaging modalities can readily identify invasion into the glossotonsillar sulcus, the intrinsic tongue, and the preepiglottic space (Fig. 17-18).1 Lateral and posterior pharyngeal wall tumors can be easily overlooked radiographically, but imaging is good for assessing deep invasion into the parapharyngeal space (Figs. 17-19 and 17-20).
Soft palate tumors require coronal imaging for adequate assessment of possible bony invasion of both the hard palate and extension through the parapharyngeal space to the skull base
(Fig. 17-21). MRI may be better for visualization of tumor extending along the tensor veli palatini and the levator veli palatini muscles to the skull base.
(Fig. 17-21). MRI may be better for visualization of tumor extending along the tensor veli palatini and the levator veli palatini muscles to the skull base.
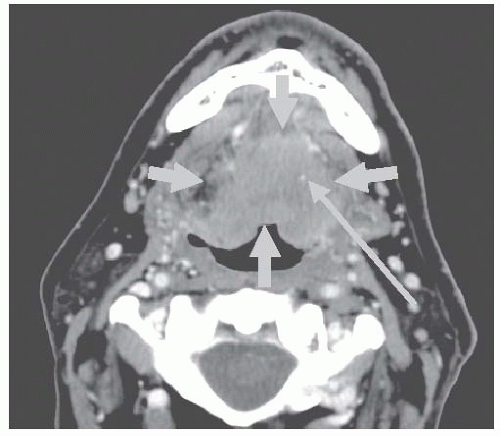 FIGURE 17-15. Axial contrast-enhanced computed tomography (CT) shows an aggressive tumor involving the tongue base (short arrows). Note that the tumor encases the lingual artery (long arrow). |
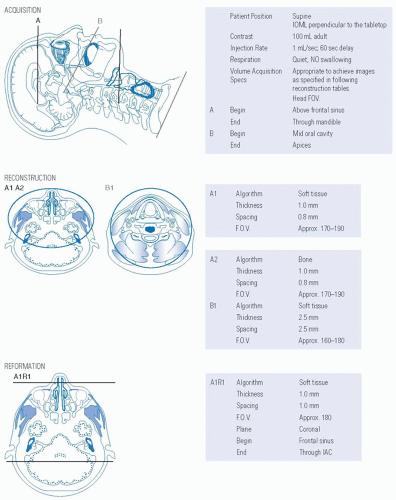 FIGURE 17-16. Protocol for computed tomography of the maxillofacial region and neck with intravenous contrast. Source: Reprinted from Mancuso AA, Hanafee WN. Head and Neck Radiology. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:2218 with permission. |
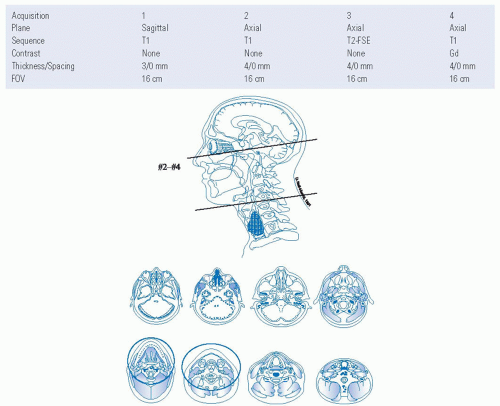 FIGURE 17-17. Protocol for magnetic resonance imaging of the oropharynx with intravenous contrast. Sourec: Reprinted from Mancuso AA, Hanafee WN. Head and Neck Radiology. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:2233 with permission. |
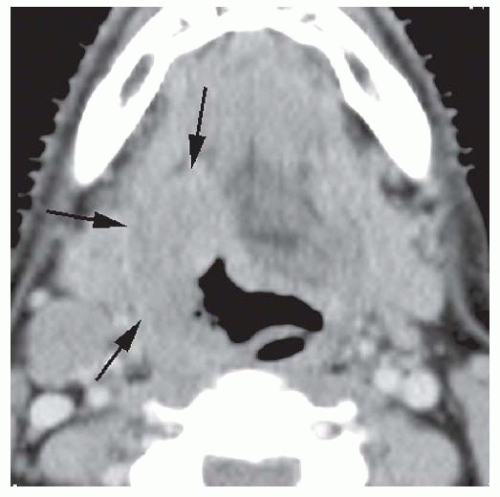 FIGURE 17-18. Axial Postcontrast CT scan shows a base of tongue cancer which extends posteriorly to invade the glossotonsillar sulcus (arrows).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





