Radiologic Imaging Concerns
Jeffrey A. Bennett
The greatest difficulty encountered with imaging of the oral cavity is artifact created by dental hardware and fillings (Fig. 16-19). CT is particularly susceptible to this beam hardening artifact which is why two separate CT acquisitions are typically obtained at different angles in an attempt to maximize soft tissue visualization. Dental artifact is less of a problem with MRI, which can generate exquisite soft tissue detail in multiple planes. The coronal is particularly useful for visualization of pathology in the oral cavity. Very thin-section CT with bone algorithm and multiplanar reformats are excellent for the detection of subtle cortical erosions caused by tumors1 (Fig. 16-20). MRI may have a slight advantage for visualization of bone marrow infiltration
by tumor, but PET/CT can also detect this finding.2 Panoramic radiographs and spot-occlusal radiographs are used particularly by dentists for the evaluation of the alveolus, teeth, and fixation plates (Fig. 16-21). Additional FDG-PET parameters are being investigated as potential markers for prognostic information and survival. These include the metabolic tumor volume and total glycolytic activity.3 The most appropriate threshold values for these variables still need to be validated. Suggested CT and MRI imaging protocols are given in Figures 16-22 and 16-23.
by tumor, but PET/CT can also detect this finding.2 Panoramic radiographs and spot-occlusal radiographs are used particularly by dentists for the evaluation of the alveolus, teeth, and fixation plates (Fig. 16-21). Additional FDG-PET parameters are being investigated as potential markers for prognostic information and survival. These include the metabolic tumor volume and total glycolytic activity.3 The most appropriate threshold values for these variables still need to be validated. Suggested CT and MRI imaging protocols are given in Figures 16-22 and 16-23.
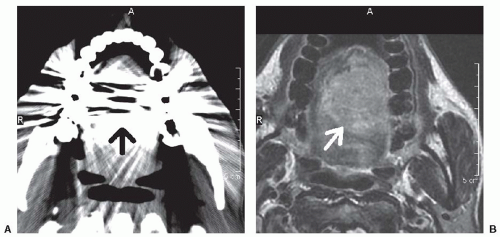 FIGURE 16-19. Axial CT scan through the oral cavity (A) is severely limited by beam hardening artifact caused by dental fillings (black arrow). The soft tissue of the oral tongue cannot be evaluated. Axial T1-weighted post gadolinium MRI (B) in the same patient shows an oral tongue enhancing squamous cell carcinoma (white arrow) and does not suffer from the same limitations as CT. |
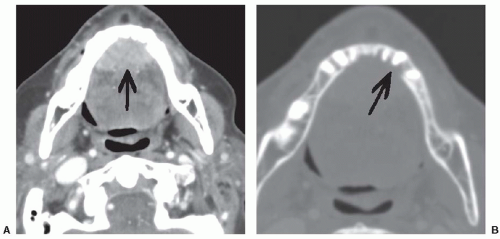 FIGURE 16-20. Axial contrast-enhanced CT scan with soft tissue windowing (A) shows an enhancing squamous cell cancer filling the anterior floor of the mouth (arrow). The same image with bone algorithm (B) shows erosion of the lingual place of the mandible (arrow) from tumor invasion into the bone. |
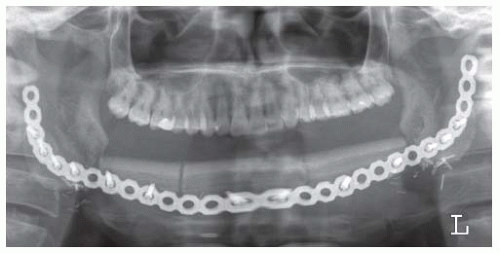 FIGURE 16-21. Panoramic radiograph is useful to assess the integrity of mandibular construct. |
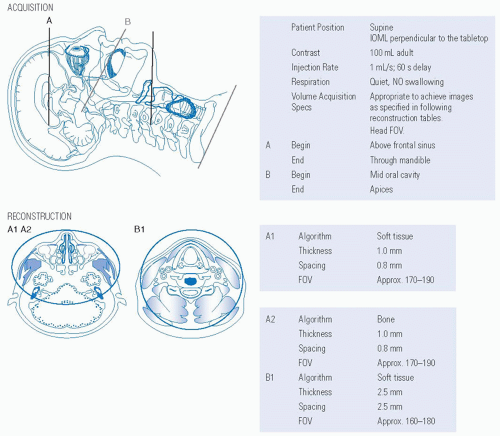 FIGURE 16-22. Protocol for CT scan of the maxillofacial region and neck with intravenous contrast. Source: Reprinted from Mancuso AA, Hanafee WN. Head and Neck Radiology. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:2218, with permission. |
ORAL TONGUE
An important observation to make on images of oral tongue lesions is whether the lesion crosses the midline lingual septum (Fig. 16-24). This affects the type of glossectomy that can be
performed. Extension into the floor of the mouth can be documented clearly with coronal CT reformatted images or coronal MRI (Fig. 16-25). Posttreatment imaging can be very helpful to evaluate lesions that cannot be directly visualized underneath the surface of flaps or underneath fibrosed scar tissue. FDG-PET can be particularly useful in these cases (Fig. 16-26).
performed. Extension into the floor of the mouth can be documented clearly with coronal CT reformatted images or coronal MRI (Fig. 16-25). Posttreatment imaging can be very helpful to evaluate lesions that cannot be directly visualized underneath the surface of flaps or underneath fibrosed scar tissue. FDG-PET can be particularly useful in these cases (Fig. 16-26).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


