Radiation Therapy Technique
William M. Mendenhall
The cervical lymph node area most often involved with cancer from an unknown head and neck primary site is level II. The most likely primary tumor sites are the base of the tongue and the tonsillar fossa. Accordingly, our philosophy has been to treat the unknown primary of the head and neck as if it were a T1 oropharyngeal cancer.1 The probable primary site and the upper neck are encompassed in equally weighted parallel-opposed fields. The field borders are the thyroid notch, the posterior spinous process of C2, the floor of the sella turcica, and 2 cm anterior to the tonsillar fossa (Fig. 15-7).2 The anterior and/or posterior borders may need to be enlarged depending on the extent of disease in the upper neck nodes. Although the likelihood of a nasopharyngeal primary is low, outside of areas where it is endemic such as Hong Kong, the risk of involved retropharyngeal nodes is relatively high, which means that part of the nasopharynx must be included in the portals.3 Modest enlargement of the portals to include the nasopharynx with a tight margin adds little morbidity and reduces the risk of recurrence in this site. The low neck is treated with an anterior portal with a tapered midline larynx block. The lateral fields are treated once daily to 64.8 Gy in 36 fractions, with a reduction of the spinal cord at 45.0 Gy. The dose to the posterior strips may be boosted on the involved side with 8 to 10 MeV electrons after the field is reduced off the cord.
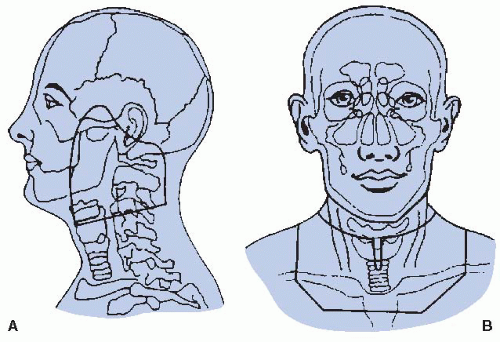 FIGURE 15-7. Radiation therapy portals used to treat head and neck mucosal sites and upper cervical lymph nodes (A) and lower cervical and supraclavicular lymph nodes (B). The inferior border for lateral portals is placed at the superoanterior border of the thyroid cartilage, shielding the hypopharynx and the larynx. Source: From Erkal HS, Mendenhall WM, Amdur RJ, et al. Squamous cell carcinomas metastatic to cervical lymph nodes from an unknown head and neck mucosal site treated with radiation therapy alone or in combination with neck dissection. Int J Radiat Oncol Biol Phys. 2001;50:55-63 (Fig. 8, p. 62), with permission. |
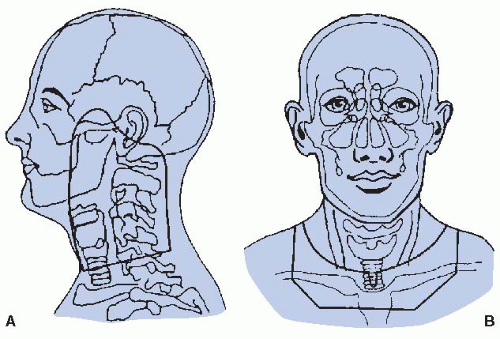 FIGURE 15-8. Radiation therapy portals used to treat head and neck mucosal sites and upper cervical lymph nodes (A) and lower cervical and supraclavicular lymph nodes (B). The inferior border for lateral portals is placed 2 cm below the inferior border of the cricoid cartilage, treating the hypopharynx and the larynx. Source: From Erkal HS, Mendenhall WM, Amdur RJ, et al. Squamous cell carcinomas metastatic to cervical lymph nodes from an unknown head and neck mucosal site treated with radiation therapy alone or in combination with neck dissection. Int J Radiat Oncol Biol Phys. 2001;50:55-63 (Fig. 8, p. 62), with permission. |
Because the occasional patient presenting with a level III node is more likely to have a hypopharyngeal or supraglottic primary cancer, these sites are included in the portals in this situation (Fig. 15-8).2
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


