Proposed Revisions to the Classification of Adenocarcinoma 5
Philip T. Cagle
Keith M. Kerr
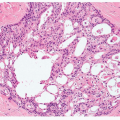
The International Association for the Study of Lung Cancer (IASLC) in collaboration with the American Thoracic Society and the European Respiratory Society is proposing an International Multidisciplinary Classification of Lung Adenocarcinoma.1 This effort is led by William Travis, chair of the 1999 and 2004 World Health Organization thoracic tumor classifications,2,3 with integrated clinical, radiologic, molecular, and surgical inputs in addition to histologic criteria. The proposed revisions to the classification of pulmonary adenocarcinomas, including bronchioloalveolar carcinomas (BACs), are partly derived from pathologic correlation with recent observations in radiology and clinical behavior and are partly in response to the needs of oncologists who are using and investigating new therapeutic protocols, including targeted molecular therapy. The observations of Noguchi and other investigators in Japan have led to the concepts of pure lepidic tumors (BAC or adenocarcinoma in situ [AIS]) and minimal invasion, which is a foundation for the new classification.4,5,6,7,8,9,10,11,12,13,14,15,16 and 17 A more precise, clinically relevant terminology is also an objective. In addition to this specific proposal, a number of authors have addressed similar issues of classification of lung cancers, particularly adenocarcinoma, in the past few years.18,19 In particular, some authors have noted that it is likely that the atypical adenomatous hyperplasia-BAC/AIS/invasive carcinoma pathway is not the only sequence of changes leading to the development of invasive adenocarcinomas.20,21
Another motivation to reconsider the classification of adenocarcinomas is the current inconsistency and multiplicity of uses of the term “bronchioloalveolar,” either as a descriptive term for a particular pattern of tumor or as an actual diagnosis, viz, bronchioloalveolar carcinoma. The term BAC is used correctly to describe localized, noninvasive, and usually nonmucinous lesions (see below and Chapters 4 and 27) but is still also frequently used in the context of both mixed pattern invasive adenocarcinomas of usual type when a BAC pattern is present and less common, multifocal advanced forms of adenocarcinoma of nonmucinous, but more often mucinous, type, where there is widespread “pneumonic consolidation” in one or both lungs by a predominantly lepidic-pattern spreading adenocarcinoma, for example, so-called “mucinous BAC.”
The increasing interest in these patterns of disease among pulmonologists and oncologists, driven by the emergence of targeted therapies that appear especially effective in some such tumors, brought the existence of widespread confusion around terminology and pathology into sharp focus. A solution was required.
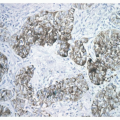
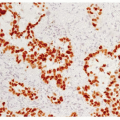
Finally, the molecular, as well as morphological, heterogeneity of lung adenocarcinomas was emphasized by a number of important publications looking at global gene expression in these tumors. A number of studies suggested subgroups of adenocarcinoma defined by common gene expression.22,23,24,25 and 26 These data were commensurate with the prospect of selecting subgroups of adenocarcinomas for specific molecular targeted therapy.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


