Prevention of Infections Related to Construction, Renovation, and Demolition in Healthcare Facilities
Prevention of Infections Related to Construction, Renovation, and Demolition in Healthcare Facilities
Russell N. Olmsted, MPH, CIC, FAPIC
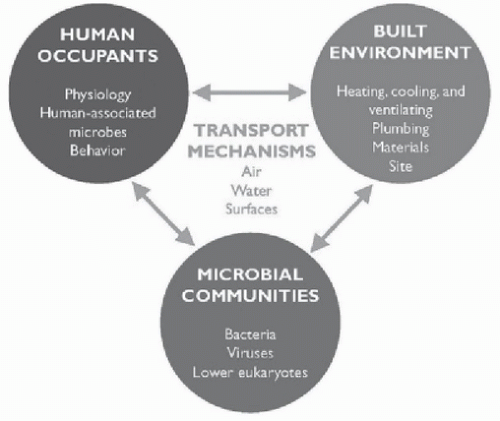
In developed countries people spend up to 90% of their lives indoors.1 Microorganisms on or in the built environments that provide this extensive exposure indoors are present in reservoirs in the air, water, soil, and inanimate surfaces as well as from human occupants. The disease risks from this near continual exposure are generally low; however, the risk assessment equation changes substantially for patients in healthcare facilities and increasingly even in residences in which people live for an extended period of time such as long-term care and assisted living. This risk is increased because of underlying diseases, conditions, therapeutic interventions, or medications that populations in healthcare environments are receiving. Interactions between people and the built environment are complex, but Figure 41-1 offers an image of the nexus between humans, the environment, and microorganisms.
Healthcare facilities are a unique ecosystem that brings together populations with unique needs/risks, centralized mechanical systems that provide heating, ventilation and air conditioning (HVAC), and potable water and specialized spaces in which a broad range of therapeutic and diagnostic procedures are provided. In addition to maintenance and support of this complex building system, the continuous use of healthcare facilities around the clock and all days of the year means that construction and renovation is a frequent reality reflecting the intense use of the built environment compared to other business occupancies in which there are regular periods of low activity and use.
No healthcare facility is an island. Each building is susceptible to unanticipated disruption of electrical power, changing environmental conditions, severe weather, and emerging social issues that compromise health of populations. Joseph Sprague, an associate member director of the American Society of Healthcare Engineers (ASHE) board of directors, captured this best when interviewed for an article on construction trends:
“Resilience is a topic that has increased in prevalence, particularly in the face of recent events, both natural and man-made,” Sprague says. “Globally, natural disasters have increased by 400 percent in the past two decades. We have also seen an increase in epidemics, including contagious diseases, diabetes and the opioid crisis. Each of these has directly and uniquely related to hospital design.”2
The investment needed to maintain healthcare facilities across the United States is ˜$40 billion per year (USD).3 Despite this investment, the average age of the existing hospital “plant” has increased by 13% over the past 10 years, and the American Hospital Association defines the average use life of a healthcare facility at 40 years.4 Therefore, construction and renovation is a constant to operating a facility. A survey of facility managers in 2019 found that 23% of respondents were involved in renovating or building acute care hospitals, and 22% indicated plans underway to accomplish this over the next 3 years.5 This compares to 20% and 18%, respectively, from a 2018 survey. A large proportion of projects underway involve centralized mechanical systems. Commenting on this Jonathan Flannery, Sr. Associate Director of advocacy for ASHE, shared,
“The growth in plumbing fixtures and piping could be the result of several factors,” Flannery says. “Hospitals might be adding more water-saving devices in light of drought conditions in some parts of the country. And some hospitals might be redoing their plumbing in response to the recent outbreaks of Legionnaires’ disease, such as removing deadend pipes or decorative water elements like fountains.”5
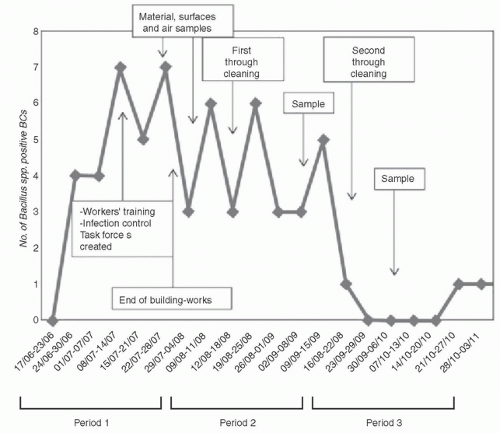
To illustrate the unique complexities of the healthcare ecosystem and continual need for maintenance, Boix-Palop and others reported a pseudo-outbreak caused by Bacillus spp.6 The epicenter of the outbreak was the Emergency Department in a large 450-bed acute care facility. Supplemental fans were deployed following mechanical failure of the HVAC supplying this space. Soon thereafter the Clinical Microbiology team noticed a significant increase in detection of Bacillus spp. from blood cultures. In addition to supplemental fans, demolition of the ED involving walls and roof was also underway without any prior notice or request for review by the infection prevention and control (IPC) team. The majority of positive blood cultures were from a single bottle and categorized as probable contaminants. The overall rate of contamination rose to 6.6% during this outbreak, and specimens from 28 unique patients detected Bacillus spp. The IPC team promptly developed infection control risk mitigation recommendations (ICRMRs) that included containment of the construction zone, improvements in blood culture collection technique, and increased cleaning and disinfection of environmental surfaces. Following these interventions, there was a notable reduction in contamination of the environment and near elimination of Bacillus spp. from blood cultures (see Fig. 41-2).
FIGURE 41-1 The complex interactions among human occupants, built environments, and associated microbial communities. (Reprinted with permission from National Academies of Sciences. Microbiomes of the Built Environment: A Research Agenda for Indoor Microbiology, Human Health, and Buildings. Washington, DC: The National Academies Press; 2017:20. https://doi.org/10.17226/23647)
FIGURE 41-2 Weekly evolution of the Bacillus spp. pseudo-outbreak. BCs, blood cultures. (From Boix-Palop L, Nicolás C, Xercavins M, et al. Bacillus species pseudo-outbreak: construction works and collateral damage. J Hosp Infect. 2017;95:118-122.)
This chapter will summarize risks to safety of patients, healthcare personnel (HCP), and visitors in healthcare facilities from construction, renovation, and demolition when there is either an absence of infection control risk assessment (ICRA) and ICRMR or ineffective separation of the active work zone from patient care areas. It will also highlight prevention strategies aimed at mitigating these risks as well as design elements that support safe, effective delivery of care.
INFECTIOUS DISEASE TRANSMISSION RISKS IN HEALTHCARE FACILITIES ASSOCIATED WITH CONSTRUCTION, RENOVATION, AND FACILITY MAINTENANCE
Sources of microorganisms in healthcare facilities include; air, water, and inanimate surfaces. Mechanically engineered systems provide for needs of building occupants and patient care; however, these also can serve as a reservoir of potential pathogens. The goal of mechanically engineered systems is dynamic flow of both air and water; however, the complexity of healthcare facilities often impedes this dynamic flow and can result in exposure and infection. These utility systems can also effect the nature and composition of microorganisms on environmental surfaces. For example, microorganisms in the potable water system can directly or indirectly contaminate work activities and products, for example, medication preparation, adjacent to outlets like plumbing fixtures. Unwanted intrusion of water from outside the facility can result in contamination of the environment. Sources of this intrusion include excessive rain, broken water supply line pipes, contractor error during renovation, or construction or inadvertent release or water by employees. If such intrusions are not mitigated in a timely manner, there is a greater risk of mold growth from saturation of cellulosecontaining materials (eg, paper facing) covering drywall (gypsum), which allow fungal spores to germinate and serve as a reservoir of possible pathogens.7
Inanimate surfaces also can serve as sources for microbes—often these are contributed by the human occupants during frequent contact between those surfaces touched with high frequency.8 Therefore, similar to humans, buildings develop their own microbiome.
According to a comprehensive review of the microbiome of the built environment by national Academy of Sciences: “The sources and reservoirs of microbes that can be found in the air and in water distributed in building systems:
Air:
Mechanical heating, ventilation, and air conditioning (HVAC) systems;
Airborne particles that have been aerosolized via HVAC operation or occupant activities, such as walking or cleaning;
Outdoor air that enters through infiltration and natural or mechanical ventilation; and
Reservoirs in unfinished spaces such as crawl spaces, basements and attics, and concealed spaces that are linked to occupied spaces via a range of airflow pathways.
Water:
Municipal or well water supplies, harvested rainwater, recycled water, and drinking fountain water;
Roof, foundation, and plumbing leaks;
Condensation on or in walls and on cold water pipes;
Mechanical equipment drain pans, coils, insulation, and filters;
Cooling towers and natural or manufactured surface ponds;
Hot water storage tanks, with subsequent aerosolization through plumbing fixtures;
Aerosolized water from personal hygiene practices (eg, showering, bathing), and toilet flushing; and
Water features, including fountains, pools, hot tubs, whirlpool baths, and spas…”9
Disruption of the built environment during construction or renovation can result in exposure and transmission of microorganisms to patients in healthcare facilities—most notably resulting in invasive fungal infections. Kanamori and others reviewed reports of outbreaks caused by fungi associated with construction and renovation published between 1974 and 2014.10 Infections caused by Aspergillus spp. were the most common and occurred predominately in larger community or university-affiliated healthcare facilities. This likely reflects the complexity of populations served and higher proportion of those who were immunocompromised from underlying diseases or therapies received. They identified 28 definite outbreaks wherein the majority resulted in invasive pulmonary aspergillosis (IPA). IPA carries a very high associated mortality that ranges between 38% and 75% and can be identified as complication of patients severely ill with preceding influenza in intensive care units (ICUs).11,12 Other pathogens causing clusters or outbreaks identified by Kanamori and others included Zygomycetes, pulmonary mucormycosis or Cunninghamella bertholletiae, and other fungi. Sixty percent of these outbreaks coincided with new construction projects followed by renovation (30%), demolition (6.3%), and excavation (4.7%). The infectious dose of IPA is exceedingly low. In some outbreaks among immunocompromised patients, this was <1 colony-forming unit (CFU)/m3. This emphasizes the critical need to contain areas or zones undergoing active construction or renovation from patient care areas. Effective strategies that accomplish this have mitigated the risk of IPA and other fungal infections from environmental reservoirs in healthcare facilities and will be discussed later in this chapter.
Mechanical HVAC systems are an integral component of operating a healthcare facility. The American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE) publishes and maintains a number of standards. One of these, Ventilation of Healthcare Facilities (ANSI/ASHRAE/ASHE Standard 170-2017), is a design standard for mechanical engineers to apply for new construction of healthcare facilities. According to ASHRAE, “The purpose of this standard is to define ventilation system design requirements that provide environmental control for comfort, asepsis, and odor in healthcare facilities.”13 This standard addresses design for HVAC system that include spaces used for surgical procedures, airborne infection isolation rooms (AIIRs), pressure relationships, temperature and relative humidity, and air exchange. By contrast, it does not address daily operations of the HVAC system led by facility managers. HVAC systems can also serve as a source of infection when the system is compromised or when preventive maintenance is neglected. According to the U.S. Centers for Disease Control and Prevention (CDC),
“Heating, ventilation, and air conditioning (HVAC) systems in healthcare facilities are designed to a) maintain the indoor air temperature and humidity at comfortable levels for staff, patients, and visitors; b) control odors; c) remove contaminated air; d) facilitate air-handling requirements to protect susceptible staff and patients from airborne healthcare-associated pathogens; and e) minimize the risk for transmission of airborne pathogens from infected patients.”
Table 41-1 summarizes disease transmission risks from HVAC systems including risk factors that lead to an increased risk of exposure to patients and personnel.
As described, potable water also can be a reservoir of a range of microorganisms and is under increased scrutiny by regulatory and accreditation agencies.15 This reflects detection of an increasing incidence of Legionnaires disease (LD) across the United States with almost a quarter of definite cases associated with exposure to healthcare facilities during the incubation period and of possible cases almost half were in healthcare facilities prior to onset of infection.16 Risk of exposure and infection in healthcare facilities reflects the convergence of populations with risk factors for LD, amplification of Legionella spp. in complex water distribution network commonly present in facilities, and inhalation of water droplets containing this bacteria produced by plumbing fixtures like shower heads. Legionella are ubiquitous in soil and freshwater lakes, but optimal growth occurs in hot water temperature that range between 25°C and 43°C. Once in water distribution loops, Legionella spp. become part of biofilms—usually living as intracellular inhabitants in protozoa. In addition, stagnant conditions in the water distribution loops in facilities from periodic inactivity in flow of water through premise plumbing or construction can perpetuate presence of this and other bacteria.
TABLE 41-1 Ventilation Hazards in Healthcare Facilities That May Be Associated With Increased Potential of Airborne Disease Transmission
Problem
Consequences
Possible solutions
Water-damaged building materials
Water leaks can soak wood, wall board, insulation, wall coverings, ceiling tiles, and carpeting. All of these materials can provide microbial habitat when wet. This is especially true for fungi growing on gypsum board.
Replace water-damaged materials.
Incorporate fungistatic compounds into building materials in areas at risk for moisture problems.
Test for all moisture and dry in <72 h. Replace if the material cannot dry within 72 h.
Filter by-passes
Rigorous air filtration requires air flow resistance. Air stream will elude filtration if openings are present because of filter damage or poor fit.
Use pressure gauges to ensure that filters are performing at proper static pressure.
Make ease of installation and maintenance criteria for filter selection.
Properly train maintenance personnel in HVAC concerns.
Design system with filters downstream from fans.
Avoid water on filters or insulation.
Improper fan setting
Air must be delivered at design volume to maintain pressure balances. Air flow in special vent rooms reverses
Routinely monitor air flow and pressure balances throughout critical parts of HVAC system.
Minimize or avoid using rooms that switch between positive and negative pressure.
Ductwork disconnections
Dislodged or leaky supply duct runs can spill into and leaky returns may draw from hidden areas. Pressure balance will be interrupted, and infectious material may be disturbed and entrained into hospital air supply.
Design a ductwork system that is easy to access, maintain, and repair.
Train maintenance personnel to regularly monitor air flow volumes and pressure balances throughout the system.
Test critical areas for appropriate air flow.
Air flow impedance
Debris, structural failure, or improperly adjusted dampers can block duct work and prevent designed air flow
Design and budget for a duct system that is easy to inspect, maintain, and repair.
Alert contractors to use caution when working around HVAC systems during the construction phase.
Regularly clean exhaust grilles.
Provide monitoring for special ventilation areas.
Open windows
Open windows can alter fan-induced pressure balance and allow dirty-to-clean air flow
Use sealed windows.
Design HVAC systems to deliver sufficient outdoor dilution ventilation.
Ensure that OSHA indoor air quality standards are met.
Dirty window air conditioners
Dirt, moisture, and bird droppings can contaminate window air conditioners, which can then introduce infectious material into hospital rooms
Eliminate such devices in plans for new construction.
Where they must be used, make sure that they are routinely cleaned and inspected.
Inadequate filtration
Infectious particles may pass through filters into vulnerable patient areas
Specify appropriate filters during new construction design phase.
Make sure that HVAC fans are sized to overcome pressure demands of filter system.
Inspect and test filters for proper installation.
Maintenance disruptions
Fan shut-offs, dislodged filter cake material contaminates downstream air supply and drain pans. This may compromise air flow in special ventilation areas.
Budget for a rigorous maintenance schedule when designing a facility.
Design system for easy maintenance.
Ensure communication between engineering and maintenance personnel.
Institute an ongoing training program for all involved staff members.
Excessive moisture in the HVAC system
Chronically damp internal lining of the HVAC system, excessive condensate, and drip pans with stagnant water may result from this problem
Locate duct humidifiers upstream of the final filters.
Identify a means to remove water from the system.
Monitor humidity; all duct take-offs should be downstream of the humidifiers so that moisture is absorbed completely.
Use steam humidifiers in the HVAC system.
Duct contamination
Debris is released during maintenance or cleaning
Provide point-of-use filtration in the critical areas.
Design air-handling systems with insulation of the exterior of the ducts.
Do not use fibrous sound attenuators.
Decontaminate or encapsulate contamination.
Adapted from CDC Healthcare Infection Control Practices Advisory Committee (HICPAC). Guidelines for Environmental Infection Control in Healthcare Facilities. 2003. https://www.cdc.gov/infectioncontrol/guidelines/environmental/index.html. Accessed May 17, 2020 Ref.14
Mermel and colleagues described an association between construction and cases of healthcare-associated LD which they postulated were related to stagnation of or disruption in normal flow of water.17 Subsequently Stout and others investigated widespread detection of Legionella pneumophila from potable water system within 1 month of completion of construction of a long-term care facilities followed by a series of healthcare-associated LD over a 2-year period.18
Unfortunately, Legionella spp. are not the only microorganisms found within potable and nonpotable water systems. Perkins and colleagues describe requests for assistance from CDC to investigate water-related detection of possible pathogens over an almost 3-year period.19 Over 20% of these requests involved waterborne microorganisms and involved over 1000 patient infections. Nontuberculous mycobacteria (NTM) accounted for the highest proportion of these (n = 40, 29.9%), with Pseudomonas spp. and Burkholderia spp. involved in 18.7% and 10.4% of all water-related investigations, respectively. NTM are particularly adapted to survival on potable water because they populate biofilms in the extensive network of water systems and are resistant to disinfectants added to drinking water including chlorine and chloramine.
Only gold members can continue reading. Log In or Register to continue
Jun 8, 2021 | Posted by drzezo in INFECTIOUS DISEASE | Comments Off on Prevention of Infections Related to Construction, Renovation, and Demolition in Healthcare Facilities
 Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
 Healthcare-Associated Infections Related to the Use of Intravascular Devices
Healthcare-Associated Infections Related to the Use of Intravascular Devices
 MDRO Infections: Gram-Positive Organisms (Including Methicillin-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococcus)
MDRO Infections: Gram-Positive Organisms (Including Methicillin-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococcus)
 Epidemiology and Prevention of Healthcare-Associated Infections Related to Animals in the Hospital
Epidemiology and Prevention of Healthcare-Associated Infections Related to Animals in the Hospital



