Chapter 45 Practical Aspects of Hematologic Stem Cell Harvesting and Mobilization
Choice of Hematologic Stem Cell Product for Transplantation
Table 45-1 Randomized Studies Comparing Marrow and PBSC as HSC Sources*
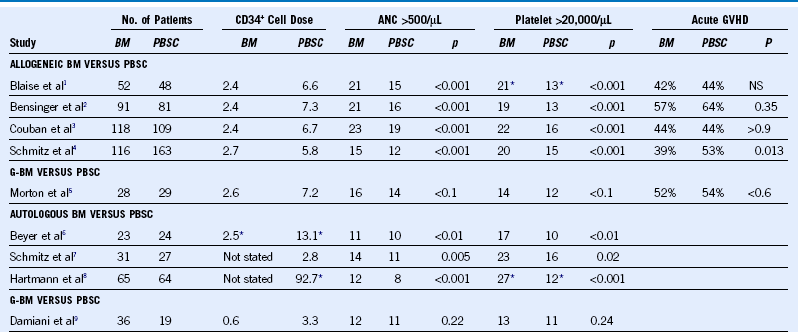
ANC, Absolute neutrophil count; BM, bone marrow, G-BM, granulocyte colony-stimulated bone marrow; NS, not significant; PBSC, peripheral blood stem cell.
Evaluation of the Marrow or Peripheral Blood Stem Cell Donor
• Education of donor, including education regarding procedures, risks, alternatives, and possible future collections
• Medical history, including special attention to history of autoimmune disorders, arthritis, cardiac and vascular diseases, and history of cancer
• History of high-risk behaviors, such as recent tattoos, body piercing, sexual practices, and travel
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


