As will be shown later in this chapter, there is strong evidence that radiation therapy (RT) can play an important role in the curative treatment of selected patients with ovarian cancer. However, the decision to use RT, particularly with curative intent, should be made only after very careful consideration of the risks and benefits of all treatment options. Unfortunately, it has been difficult to achieve a cohesive strategy for the use of RT for ovarian cancer, for a number of reasons:
Most patients with ovarian cancer either have or are at high risk for developing intra-abdominal carcinomatosis and are therefore not good candidates for definitive local treatment.
Although RT was once strongly considered in the initial treatment of patients with minimal or no gross disease, the development of more effective chemotherapy and the adverse effects of early RT methods led to a decline in the use of RT for this indication. Eventually, many gynecologic oncologists entirely abandoned the use of RT for definitive treatment.
RT is often considered only as a treatment of last resort, offered after the patient has already undergone several operations and many courses of chemotherapy. These previous treatments increase the risk of major radiation-related complications, narrowing the therapeutic window for complication-free definitive treatment.
More than 20 years have passed since the role of RT for ovarian cancer was last investigated in a large prospective trial. Although retrospective studies suggest that RT may have a role in selected patients, radiation treatment methods have been inconsistent, making it difficult to formulate definitive recommendations.
The case studies at the end of this chapter demonstrate that some patients enjoy long disease-free intervals and may even be cured after receiving RT for localized recurrence of ovarian cancer. Furthermore, population-based studies suggest that certain subsets of patients with ovarian cancer might benefit sufficiently from adjuvant RT to justify its use in the initial management of their disease. However, RT for ovarian cancer remains highly controversial. To understand how RT can contribute to the management of ovarian cancer, radiation oncologists must understand the natural history of this disease and be familiar with surgery and chemotherapy options and their expected outcomes.
PRESENTATION AND PATTERNS OF SPREAD
The typical presenting symptoms of ovarian cancer are pain, dysuria, bloating, and early satiety. These symptoms are often vague and may not occur until the cancer is already advanced. At diagnosis, about 70% of patients have disease that has extended or metastasized beyond the ovary.
Disease is bilateral at diagnosis in 25% to 30% of cases. Ovarian cancer may extend directly from the ovary to the rectosigmoid, ureters, pelvic sidewall, or other adjacent tissues. The most common form of metastasis from ovarian cancer is transcoelomic metastasis, in which detached malignant cells following the pattern of flow of peritoneal fluid implant on peritoneal surfaces and form metastatic growths. Common sites of involvement resulting from this type of metastasis are the pelvic cul-de-sac (rectouterine pouch), omentum, paracolic gutters, and undersurface of the right hemidiaphragm. However, not all patients with malignant cells found in peritoneal fluid have or develop peritoneal tumor involvement, suggesting that not all cancers have the capacity to implant and grow on serosal surfaces.
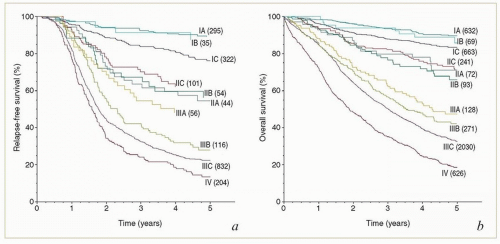
FIGURE 14.1 Relapse-free survival (a) and overall survival (b) of patients with epithelial ovarian cancer by FIGO substage. Stage categories in this figure refer to the 2006 FIGO stage categories. (From Heintz AP, Quinn MA, Benedet JL, et al. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet. 2006;95(suppl 1):S161-S192.)
Ovarian cancer can spread directly to pelvic, paraaortic, or occasionally, inguinal lymph nodes (Chapter 5). Lymphadenectomy series indicate that 50% to 80% of patients with stage III or IV disease and at least 20% of patients who would otherwise be classified as having stage I or II disease have pelvic or paraaortic lymph node metastases.1
Hematogenous metastases are present in only 2% to 3% of patients at diagnosis. About one-third of patients with stage III or IV disease at diagnosis eventually develop metastases in the lung, liver, brain, bone, subcutaneous tissues, or other sites.
PROGNOSTIC FACTORS
FIGO Stage
The FIGO staging system is based on clinical findings and on the results of intra-abdominal surgical exploration. Both recurrence-free survival (Fig. 14.1) and overall survival are strongly correlated with FIGO stage.2 However, about half of all patients have stage III disease, and most of those have stage IIIC disease (Fig. 14.2).
In 2014, FIGO published a revised staging system for ovarian cancer (Table 14.1).3 In this new version, ovarian, fallopian tube, and primary peritoneal cancers were for the first time covered by a single staging system, reflecting the similar natural histories and approaches to treatment for carcinomas arising in these sites. Also, the stage IC category was subdivided to reflect findings concerning the relationships between tumor spill and outcome.
However, the most significant changes in the 2014 FIGO staging system involved the classification of ovarian cancer with nodal metastases. In the 2006 FIGO staging system, all cases with lymph node metastases were classified as at least stage IIIC. Since then, retrospective studies demonstrated that patients who had pelvic or aortic lymph node metastases without peritoneal carcinomatosis had a better prognosis than other patients with stage IIIC disease.1,4 For this reason, in the 2014 system, FIGO designated a separate category (stage IIIA1) for pelvic or aortic nodal metastases without peritoneal carcinomatosis. For radiation oncologists, this separate designation for apparently locoregionally confined disease will help to clarify the initial distribution of disease when patients are referred for treatment of subsequent recurrences.
FIGURE 14.2 Distribution of patients with newly diagnosed epithelial ovarian cancer by FIGO stage. Stage categories in this figure refer to the 2006 FIGO stage categories. (Data from Heintz AP, Quinn MA, Benedet JL, et al. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet. 2006;95(suppl 1):S161-S192.)
TABLE 14.1 FIGO Staging for Primary Cancers of the Ovary, Fallopian Tube, and Peritoneum (Effective January 1, 2014)
Stage I
Tumor confined to ovaries or fallopian tubes
IA
Tumor limited to one ovary (capsule intact) or fallopian tube; no tumor on ovarian or fallopian tube surface; no malignant cells in ascites or peritoneal washings
IB
Tumor limited to both ovaries (capsule intact) or fallopian tubes; no tumor on ovarian or fallopian tube surface; no malignant cells in ascites or peritoneal washings
IC
Tumor limited to one or both ovaries or fallopian tubes, with any of the following:
IC1
Surgical spill intraoperatively
IC2
Capsule ruptured before surgery or tumor on ovarian or fallopian tube surface
IC3
Malignant cells in ascites or peritoneal washings
Stage II
Tumor involves one or both ovaries or fallopian tubes with pelvic extension (below the pelvic brim) or primary peritoneal cancer
IIA
Extension and/or implants on the uterus, fallopian tubes, or ovaries
IIB
Extension to other pelvic intraperitoneal tissues
Stage III
Tumor involves one or both ovaries or fallopian tubes or peritoneal cancer, with cytologically or histologically confirmed spread to the peritoneum outside the pelvis or metastasis to the retroperitoneal lymph nodes
IIIA
Metastasis to the retroperitoneal lymph nodes with or without microscopic peritoneal involvement beyond the pelvis
IIIA1
Positive retroperitoneal lymph nodes only (histologically proven), either ≤10 mm in greatest dimension (IIIA1i) or >10 mm (IIIA1ii)
IIIA2
Microscopic extrapelvic (above the pelvic brim) peritoneal involvement with or without positive retroperitoneal lymph nodes
IIIB
Macroscopic peritoneal metastases beyond the pelvic brim ≤2 cm in greatest dimension with or without metastases to retroperitoneal nodes
IIIC
Macroscopic peritoneal metastases beyond the pelvic brim >2 cm in greatest dimension, with or without metastases to retroperitoneal nodes
Metastases to extra-abdominal organs (including inguinal lymph nodes and lymph nodes outside of the abdominal cavity)
In the 2014 staging system, FIGO also shifted isolated inguinal node metastases from stage IIIC to stage IVB. There are few data documenting the outcomes of patients with this rare presentation; however, the groin is a primary echelon site of lymphatic drainage from the ovaries (Chapter 5), and anecdotal reports of prolonged survival after local treatment for isolated groin recurrences (CS 14.8)5 suggest that the prognosis may not be as grave as the stage IVB designation suggests.
Histologic Subtype
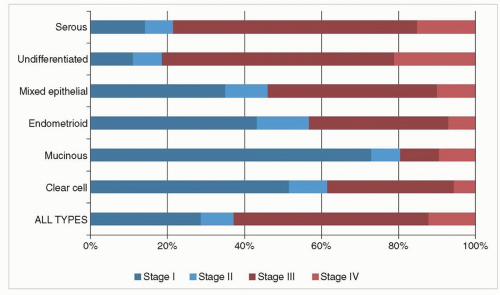
The stage of ovarian cancer at presentation is strongly correlated with the histologic subtype (Fig. 14.3).2 Differences in the behaviors of these subtypes provide important insights for clinicians interested in defining the role of local treatment in the management of ovarian cancer.
Because about two-thirds of ovarian cancers are serous, undifferentiated, or of mixed histologic subtype with a serous component, the behavior of these cancers dominates clinical impressions of the disease. Serous carcinomas, whether they originate in the ovary, fallopian tube, uterus, or peritoneum, have a strong predilection for transcoelomic spread. Although a small subset of ovarian serous cancers may lack the ability to implant on peritoneal surfaces (CS 14.3, 14.4, and 14.7), approximately 80% of patients with ovarian serous cancer present with advanced disease, usually with abdominal carcinomatosis. Undifferentiated cancers and carcinosarcomas exhibit similarly aggressive behaviors.
Mucinous, clear cell, and endometrioid cancers are much less likely to spread intraperitoneally; about two-thirds of these cancers are confined to the pelvis at diagnosis (Fig. 14.3). Several authors have reported that locoregionally confined ovarian cancers of these subtypes have a relatively good prognosis after treatment with involved-field RT.5,6,7 As data accumulate, it will also be interesting to note whether patients with these subtypes are more likely to present with isolated pelvic or aortic lymph node metastases (i.e., stage IIIA1 disease).
FIGURE 14.3 Relationship between histologic subtype and FIGO stage in patients with epithelial ovarian cancer. Stage categories in this figure refer to the 2006 FIGO stage categories. (Data from Heintz AP, Quinn MA, Benedet JL, et al. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet. 2006;95(suppl 1):S161-S192.)
Patients with early-stage (FIGO stage I or II) serous, mucinous, and clear cell carcinomas have similar prognoses. However, mucinous and clear cell carcinomas tend to respond more poorly to chemotherapy than other histologic subtypes, and therefore, patients with advanced mucinous or clear cell carcinomas have a relatively poor prognosis.2 Because mucinous and clear cell cancers have a greater tendency to remain localized and have relatively poor chemoresponsiveness, patients with these cancers are relatively good candidates for RT under appropriate circumstances.
Grade
In general, patients with ovarian cancer with grade 1 tumors tend to survive longer than patients with grade 2 or 3 tumors of similar stage,2 although studies have demonstrated significant inter- and intraobserver variation in the assignment of tumor grade.
ROLES OF SURGERY AND CHEMOTHERAPY
Surgery and chemotherapy are the cornerstones of treatment for epithelial ovarian cancer. While RT can play an important role in individual cases, it can only be recommended after careful consideration of the risks and potential benefits of all available treatments. For this reason, the roles of surgery and chemotherapy in patients with early-stage, advanced, and recurrent ovarian cancer are reviewed here.
Surgery
Early-Stage Disease
In a patient with an adnexal mass, the first step in management is to assess the risk of malignancy using pelvic ultrasonography and measurement of the serum CA-125 level. If the findings are suggestive of malignancy, the patient should be referred to a gynecologic oncologist for surgical evaluation. If intraoperative frozen section is positive for invasive ovarian cancer, full surgical staging should be performed.8
The standard surgical treatment and evaluation for early-stage ovarian cancer includes total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO) (ideally with intact removal of the ovarian tumor), omentectomy, and pelvic and paraaortic lymph node dissection. Peritoneal surfaces should be explored, and suspicious lesions should be biopsied. In addition, random biopsies of the cul-de-sac, paracolic gutters, intestinal mesenteries, and diaphragm should be performed, and ascitic fluid or pelvic washings should be collected.
A horizontal suprapubic (Pfannenstiel) incision does not provide adequate access for the evaluation of the upper abdomen; studies of patients who have had re-exploration through a more appropriate midline incision reveal that the stage is increased as a result in at least 30% of those initially thought to have stage I or II disease.9
Advanced Disease
Patients with more advanced disease who are medically fit and who do not have metastases in organ parenchyma usually undergo initial cytoreductive surgery, including TAHBSO, omentectomy, lymph node dissection, and resection of as much metastatic disease as possible; the goal of surgery is to achieve an optimal cytoreduction leaving no more than microscopic residual disease.8
Cytoreductive surgery typically provides immediate benefit by relieving gastrointestinal symptoms caused by intestinal compression or obstruction, thereby improving the patient’s overall nutritional status. A number of more theoretical benefits of cytoreductive surgery include removal of poorly vascularized regions that might not receive adequate concentrations of chemotherapy; reduction in the proportion of nonproliferating, relatively chemoresistant cells; reduction in the proportion of hypoxic cells; and reduction (potentially by several logs) in the overall number of cancer cells that must be killed by chemotherapy. However, the prognosis of patients with bulky (>10 cm) metastatic deposits or extensive carcinomatosis remains poor even after an optimal cytoreduction.8
Patients with advanced disease who, for medical or other reasons, are unable to undergo primary cytoreductive surgery typically have a diagnosis made by biopsy and then receive 3 or more cycles of neoadjuvant chemotherapy. If repeat evaluation after neoadjuvant chemotherapy demonstrates a satisfactory initial response, the patient usually undergoes an interval debulking surgery with the goal of achieving an optimal cytoreduction before administration of additional chemotherapy.
There is fairly strong evidence that achievement of optimal primary cytoreduction, which requires effort and skill, is associated with improved survival rates; however, the poorer survival rates of patients with suboptimal cytoreduction may, in part, reflect confounding adverse prognostic factors.2,10
Recurrent Disease
Surgery performed to achieve optimal cytoreduction of disease that has recurred after chemotherapy is termed secondary cytoreduction. Patients whose cancer progresses or recurs within 6 months of the completion of platinum-based chemotherapy (i.e., platinum-resistant cancer) do not appear to benefit from secondary cytoreduction. However, retrospective studies indicate that secondary cytoreduction may benefit selected patients with relatively late, localized recurrences that can be completely resected.
Additional notes about surgery for ovarian cancer.
Although lymph node dissections are increasingly being included in routine surgical staging, these are often limited nodal samplings; a thorough lymphadenectomy, which adds significantly to the length and potential adverse effects of surgery, is frequently not performed.
There has been a move toward increasingly thorough surgical staging, which has improved the quality of information used to select treatments but has also resulted in stage migration toward more advanced stages, causing improvements in survival to appear more encouraging when viewed stage by stage than when examined for the overall population.2
A 2012 SEER analysis found that 48% of patients undergoing surgical staging for ovarian cancer have at least one perioperative complication. The ˜16% of patients who had multiple complications were more likely to have delayed initiation of chemotherapy and a poor outcome.11
Cytoreductive surgeries are often long, open operations that involve bowel resections, ureterolysis, extensive lymph node dissections, and other procedures that traumatize critical structures. These surgical manipulations undoubtedly contribute to the risk of adverse effects from subsequent RT.
Chemotherapy
The current standard chemotherapy for most patients with newly diagnosed epithelial ovarian cancer is combination chemotherapy including a platinum compound (usually carboplatin) and a taxane (usually paclitaxel). Patients who have early-stage disease may be treated with combination chemotherapy or with carboplatin only. The only patients for whom chemotherapy is not recommended are those with FIGO (2014) stage IA or IB, grade 1 disease.8 A brief review of the studies leading to this standard will help to put the evolving role of RT for ovarian cancer in context.
Early-Stage Disease
Adjuvant chemotherapy is usually recommended for patients who have stage IC or II disease or grade 2 or 3 disease of any stage.8,12 Although there is no definitive evidence that chemotherapy improves survival in patients with early-stage disease who have had thorough surgical staging, recent studies suggest that some patients with early-stage disease may derive greater benefit from adjuvant chemotherapy than others.
In the late 1980s, three trials that compared combination chemotherapy (cisplatin and cyclophosphamide) with either observation or intraperitoneal instillation of phosphorus 32 demonstrated lower recurrence rates for patients who received adjuvant chemotherapy but no differences in overall survival rates.13,14
In the 1990s, two large European randomized trials compared platinum-based chemotherapy with observation in patients with early-stage disease.15 Although both trials demonstrated significant improvements in survival for patients who received chemotherapy, many of the patients in these trials did not have optimal surgical staging. When a subset analysis was performed that was limited to patients who had optimal surgical staging, no significant survival improvement was seen with chemotherapy.11,15
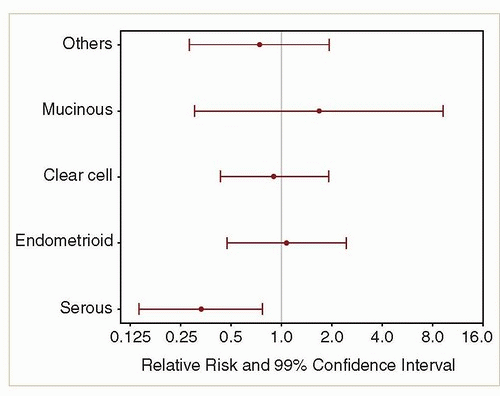
In a subsequent Gynecologic Oncology Group (GOG) trial (GOG-157),16 there was no difference in outcome for 3 versus 6 cycles of carboplatin and paclitaxel in patients with earlystage, high-risk (stage IA, grade 3; stage IB, grade 3; clear cell; or any stage IC or II) epithelial ovarian cancer. Interestingly, an exploratory subset analysis showed that for 97 patients with serous carcinomas, the recurrence rate was significantly less for patients randomized to receive 6 cycles,17 whereas for 266 patients with endometrioid, clear cell, or mucinous cancers, the number of cycles had no influence on the recurrence rate, providing additional evidence of the different behavior of these subtypes (Fig. 14.4).
FIGURE 14.4 Relative risk of recurrence for 427 patients with ovarian cancer who received 6 versus 3 cycles of carboplatin and paclitaxel in GOG-157 by histologic subtype. (From Chan JK,Tian C, Fleming GF, et al. The potential benefit of 6 vs. 3 cycles of chemotherapy in subsets of women with early-stage high-risk epithelial ovarian cancer: an exploratory analysis of a Gynecologic Oncology Group study. Gynecol Oncol. 2010;116(3):301-306, doi:10.1016/j.ygyno.2009.10.073.)
Advanced Disease
Dozens of prospective randomized trials conducted over more than 40 years have led to the current standard treatments for advanced ovarian cancer. Although these studies have led to some incremental improvements, most patients with advanced disease eventually die of causes related to ovarian cancer (Fig. 14.1).2
In the 1970s, the standard treatment for ovarian cancer was single-agent chemotherapy with alkylating agents such as melphalan, cyclophosphamide, or chlorambucil. Investigators sought to improve outcomes by combining these agents with other available cytotoxic drugs, but more than a dozen trials failed to improve on the results achieved with single agents.18 At the time, patients who had minimal residual disease after surgery often had pelvic RT added to alkylating agent therapy. Two trials that compared this standard with whole abdominal RT are discussed in the section “Historical Evidence of Benefit from RT” later in this chapter.
After cisplatin was made available for clinical use in the late 1970s, it was soon demonstrated to be superior to cyclophosphamide as a single agent, increasing the median survival of patients with advanced disease from 12 to 19 months.19 A meta-analysis of trials that tested combinations that did or did not include cisplatin also suggested a benefit from cisplatin treatment.20 However, randomized trials comparing cisplatin alone or in combination with other agents yielded inconclusive results.20
In the late 1980s, two drugs were introduced that would eventually form the backbone of ovarian cancer treatment: carboplatin and paclitaxel. Carboplatin, introduced in 1989, was found to be as effective as cisplatin but with less nephrotoxicity and fewer gastrointestinal toxic effects20; it soon replaced cisplatin in the treatment of ovarian cancer. In the early 1990s, two large prospective trials compared a combination of carboplatin and paclitaxel with the then-standard regimen of carboplatin and cyclophosphamide; both trials demonstrated significantly improved response rates, progression-free survival, and eventually, overall survival for the paclitaxel-containing combination.21 Combinations of carboplatin and paclitaxel have continued to form the standard primary treatment for ovarian cancer for 20 years.
Several studies have tried to improve on the results seen with carboplatin and paclitaxel by adding new agents.
Addition of other cytotoxic agents. A massive 5-arm multinational trial added topotecan, liposomal doxorubicin, or gemcitabine to the carboplatin-paclitaxel backbone in various combinations. None of these combinations improved upon the 2-drug control treatment.22
Addition of bevacizumab. Two large randomized trials failed to demonstrate improved survival with addition of concurrent or maintenance bevacizumab to the combination of carboplatin and paclitaxel.23,24 One study showed a 2-month delay in time to progression, but the progression-free survival curves converged a few months after maintenance bevacizumab was discontinued.24 This minimal gain, coupled with the cost and toxic effects of bevacizumab, has prevented the drug from becoming standard for initial treatment of ovarian cancer, although it is sometimes used to treat recurrence.
Perhaps more successful have been efforts to improve outcome by increasing treatment intensity. Recent studies have focused on two methods of dose intensification: intraperitoneal chemotherapy and dose-dense chemotherapy.
Intraperitoneal chemotherapy. Several randomized trials have demonstrated significantly improved survival rates with the combination of intraperitoneal and intravenous administration of chemotherapy.25 The benefits of this approach appear to be greater for patients who have had optimal cytoreduction and less for patients with mucinous, clear cell, and low-grade tumors. Intraperitoneal chemotherapy is associated with increased toxic effects, including bowel adhesions, and may be associated with an increase in the rate of adhesion-related bowel obstruction.26 There are very few data available on the risks of RT after intraperitoneal chemotherapy, but this form of chemotherapy should be considered a possible risk factor for post-RT bowel complications.
Only gold members can continue reading. Log In or Register to continue