OSTEOPENIA IN CHILDHOOD
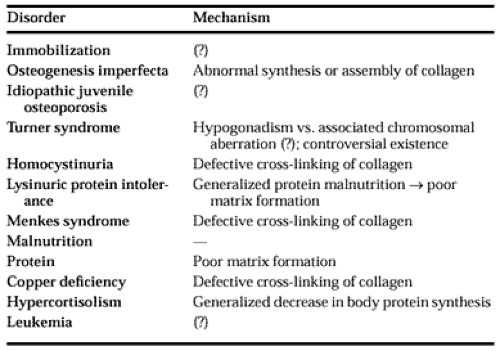
Children occasionally come to the physician’s attention because of osteopenia (radiographic evidence of reduced bone mass). Abnormalities in serum calcium, phosphorus, or alkaline phosphatase may confirm the suspicion of rickets. In less clear cases, however, differentiation between osteomalacia (defective mineralization of osteoid) and osteoporosis (decreased organic and calcified bone mass) must be sought (see Chap. 55 and Chap. 64). This discussion is concerned primarily with disorders in which osteopenia is a presenting feature (Table 70-3). There are several conditions in which osteopenia may be an associated finding and not the primary manifestation of the disease (e.g., thyrotoxicosis, acromegaly, hypogonadism [Klinefelter syndrome, Noonan syndrome, hyperprolactinemia], hyperparathyroidism, diabetes mellitus, the lactating adolescent, heparin therapy, mastocytosis, increased erythropoiesis, Down syndrome, Wilson disease, cystic fibrosis, familial dysautonomia, anorexia nervosa, and other severe chronic diseases).
 |
It appears that racial differences in bone mass begin at an early age. Adequate but not excess calcium intake in children may have positive effects on bone mineral status in adulthood.
MAJOR CHILDHOOD OSTEOPENIA
IMMOBILIZATION
Severe trauma, myelodysplasia, and juvenile rheumatoid arthritis are predisposing conditions for immobilization-related osteoporosis in children.
OSTEOGENESIS IMPERFECTA
Osteogenesis imperfecta, a heterogeneous group of diseases, has an estimated incidence of 1 per 15,000 live births. The osteopenia results from abnormal production of bone matrix secondary to defective collagen synthesis or assembly.36 Other tissues that
contain collagen may be affected, as evidenced by joint laxity and thin skin. The sclerae may appear blue because of thinning, allowing the blue pigment of the choroid to be transmitted. Improper formation of dentin may occur, and teeth may be yellow or opalescent and chip easily. Sensorineural or conductive hearing loss may be present. The skeleton is variably affected. Wormian bones (islands of bone with a rich vascular supply) are frequently observed on skull radiographs. Biochemical findings are nonspecific; however, mild hypercalcemia and hypercalciuria may be present in younger patients. Markers of bone turnover—such as serum alkaline phosphatase activity and osteocalcin as well as urinary excretion of resorptive markers—may also have higher than average values. Serum PTH and vitamin D metabolites are nearly always normal.
contain collagen may be affected, as evidenced by joint laxity and thin skin. The sclerae may appear blue because of thinning, allowing the blue pigment of the choroid to be transmitted. Improper formation of dentin may occur, and teeth may be yellow or opalescent and chip easily. Sensorineural or conductive hearing loss may be present. The skeleton is variably affected. Wormian bones (islands of bone with a rich vascular supply) are frequently observed on skull radiographs. Biochemical findings are nonspecific; however, mild hypercalcemia and hypercalciuria may be present in younger patients. Markers of bone turnover—such as serum alkaline phosphatase activity and osteocalcin as well as urinary excretion of resorptive markers—may also have higher than average values. Serum PTH and vitamin D metabolites are nearly always normal.
Numerous mutations in genes encoding the α1 and α2 chains of type I collagen (bone collagen) have been described.36a Most kindreds are affected with unique mutations, and sporadic mutations are not uncommonly reported. Studies note variable severity associated with the mutations, being dependent on the region of the gene in which the mutation occurs; thus a “regional model” for site of mutation/severity has been proposed.37 Mutations in introns resulting in abnormal mRNA processing have been described; these result in abnormal ratios of chain production, not abnormal chains, per se.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


