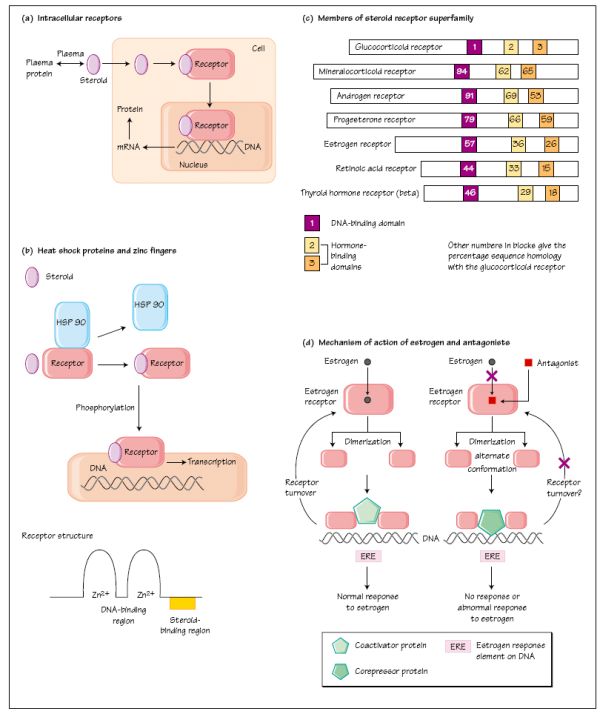
Estrogen stimulates the proliferation of breast cancer tissue and exposure to estrogens may be important in the pathogenesis of this disease. During the treatment of women with breast cancer it is routine practice to establish the presence (ER +ve) or absence (ER -ve) of estrogen receptors in cancer cells. Women who have ER +ve tumours are more likely to respond to endocrine manipulation following surgery and/or chemotherapy (50-60% response rate in ER +ve cancers, 5-10% in ER -ve tumours). The most commonly used endocrine therapy is the drug tamoxifen which has estrogenantagonist effects in the breast, probably mediated by the recruitment of corepressors for estrogen receptor action. It produces a significant fall in tumour recurrence and death rates for women with ER + ve disease, irrespective of age. The possible use of tamoxifen and the newer, selective estrogen receptor modulator drugs (SERMs, e.g. raloxifene, toremifine) for the prevention of breast cancer are under investigation. Trastuzumab, a humanized IgG1 against human epidermal growth factor receptor-2 (HER-2+), is now used to treat early breast cancer that overexpresses HER-2.
Lipophilic hormones, such as steroids and the thyroid hormones, pass easily through the plasma membrane into the cell, where they combine with specific receptor proteins (Fig. 4a). In the inactive state, for the subfamily of glucocorticoid, progesterone, estrogen and androgen receptors, the receptor is bound to a heat shock protein (HSP 90; Fig. 4b).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


