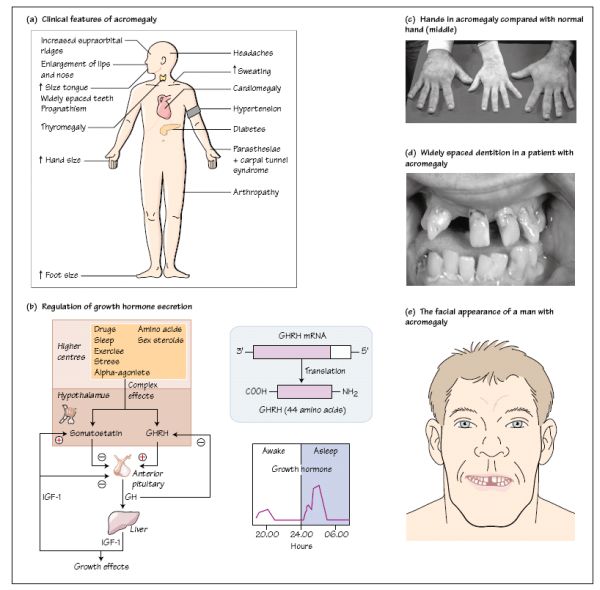
Excess growth hormone (GH) secretion causes the typical syndrome of acromegaly. Mr SJ was a 53-year-old chef who had generally been well and rarely went to the doctor. On this occasion he presented to his GP because of aches and pains in the joints of his hands which were causing a problem with his work. The GP thought he looked acromegalic and asked him a series of questions related to his symptoms, following which he established a number of abnormalities on examination. He referred Mr SJ to the local Endocrine Clinic where biochemical investigations confirmed the diagnosis of acromegaly. In particular, his plasma GH level was elevated at 25mcg/L and failed to suppress during a glucose tolerance test and his plasma IGF-1 concentration was five times the upper limit of normal. An MRI scan of the pituitary revealed a pituitary macroadenoma rising out of the pituitary fossa into the suprasellar space but not compressing the optic chiasm. He had a good response to pituitary surgery and subsequent radiotherapy, with resolution of many of the features of acromegaly. The clinical features of acromegaly are shown in Fig. 12a.
Regulation of growth hormone secretion
Growth hormone (GH) secretion is regulated primarily by the hypothalamus, which produces growth hormone-releasing hormone (GHRH; Fig. 12b). This action is integrated with the action of a hormone called ghrelin,
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


