Large Cell Carcinoma
Timothy Craig Allen
Large cell carcinoma of the lung is defined as “an undifferentiated non-small cell carcinoma that lacks the cytological and architectural features of small cell carcinoma and glandular or squamous differentiation.’1,2,3,4 and 5 Making up fewer than 10% of lung carcinomas, these poorly differentiated, generally large peripheral carcinomas often invade the pleura and chest wall.1,2,3,4 and 5 More frequently identified in men, large cell carcinomas are smoking related and present clinically and radiologically as do other non-small cell carcinomas.1-5 Besides basaloid carcinoma and large cell neuroendocrine carcinoma, there are three other extremely uncommon variants of large cell carcinoma, including clear cell carcinoma, lymphoepithelioma-like carcinoma, and large cell carcinoma with rhabdoid phenotype.1,2,3,4,5 and 6 Prior terms used to designate large cell carcinoma, such as large cell undifferentiated carcinoma and large cell anaplastic carcinoma, should be avoided.1-3 Clinically and radiologically, large cell carcinomas present in a similar manner as other non-small cell lung cancers.1-3,7 Although large cell carcinomas are generally peripheral tumors and may undergo core needle biopsy, the criteria for diagnosis require extensive tissue sampling to be fulfilled. As such, the diagnosis of large cell carcinoma is one that is reliably rendered only upon excision of, and close pathologic examination of, the tumor mass.1,5 Cytology and small biopsy specimens are generally not suitable for the diagnosis. The more general diagnosis of non-small cell carcinoma should be rendered for small biopsies or cytology specimens containing tumor cells containing features of large cell carcinoma.5 Prognostically, large cell carcinomas behave similarly to other non-small cell carcinomas.
LARGE CELL CARCINOMA, CYTOLOGY
Cytologically, large cell carcinomas usually show features that are not specific for the diagnosis of large cell carcinoma, including tumor cells arranged singly and in syncytial groups, with indistinct but generally abundant cytoplasm and large round to oval nuclei with irregular course nuclear chromatin (Fig. 8-1).1,3,4 Tumor cells often contain large, often multiple, nucleoli.
LARGE CELL CARCINOMA, GROSS FEATURES
LARGE CELL CARCINOMA, HISTOLOGY
Histologically, tumor cells are generally arranged in nests and sheets of large polygonal cells with a moderate amount of cytoplasm and nuclear features similar to the cytologic description above.1-5 Large cell carcinoma tumor cells are generally large, polygonal cells with large, hyperchromatic nuclei and conspicuous nucleoli (Fig. 8-4). H&E stain shows no adenocarcinomatous or squamous differentiation, specifically, no single-cell keratinization, keratin pearls, intercellular bridges, or acinar, papillary, or tubular structures.1-5 Mucin stain is typically negative (Fig. 8-5). While
occasional mucin droplets may be identified by mucin stain, if by PAS with diastase digestion or mucicarmine stain there are >5 mucin droplets per 2 high-power fields, then the diagnosis of solid adenocarcinoma with mucin formation is appropriate.4
occasional mucin droplets may be identified by mucin stain, if by PAS with diastase digestion or mucicarmine stain there are >5 mucin droplets per 2 high-power fields, then the diagnosis of solid adenocarcinoma with mucin formation is appropriate.4
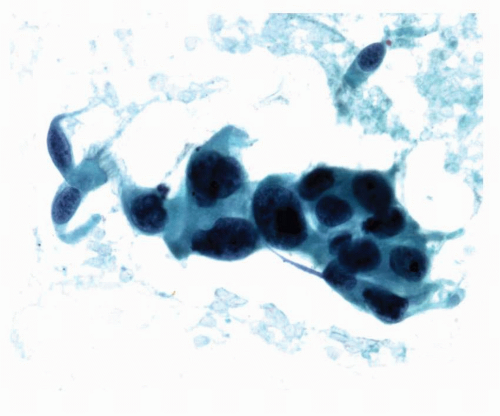 FIGURE 8-1 High-power image of Papstained fine-needle aspiration cytology of a patient who on surgical resection was found to have large cell carcinoma showing a group of tumor cells with a moderate amount of indistinct cytoplasm and large round to oval nuclei containing irregular course nuclear chromatin and occasional large nucleoli. Some benign ciliated mucosal cells are present and provide size comparison. These cytologic features are not specific for large cell carcinoma and would be appropriately diagnosed as non-small cell carcinoma. |
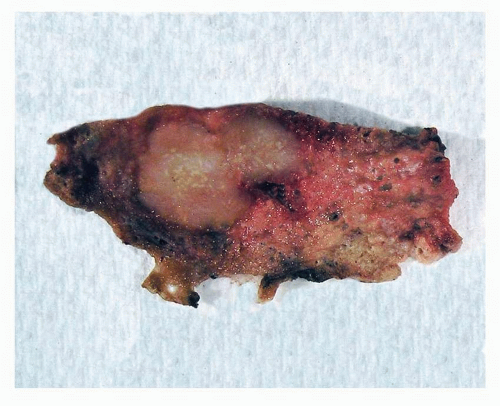 FIGURE 8-2 Gross image of a wedge resection of large cell carcinoma, showing an off-white to gray subpleural mass without areas of necrosis. |
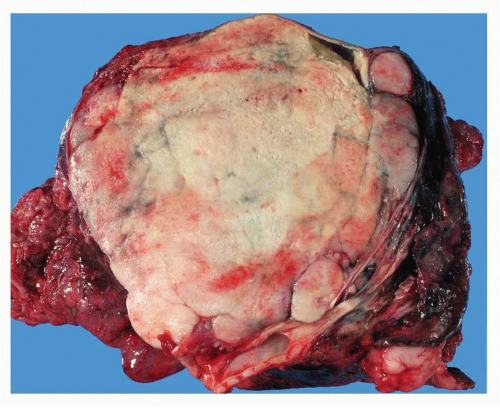 FIGURE 8-3 Gross image of a lobectomy specimen containing large cell carcinoma, with focal hemorrhage, but no cavitation seen in this large tumor mass. |
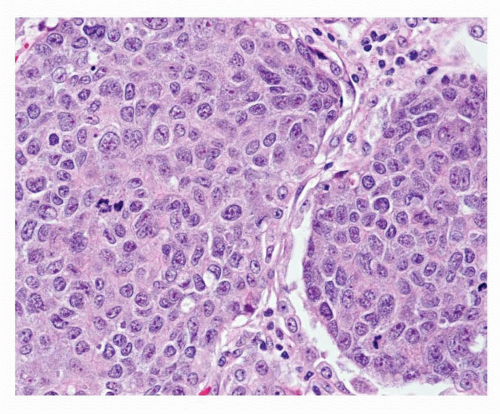 FIGURE 8-4 High-power image of large cell carcinoma showing nests of large polygonal cells with a moderate amount of cytoplasm and large, hyperchromatic nuclei with conspicuous nucleoli. |
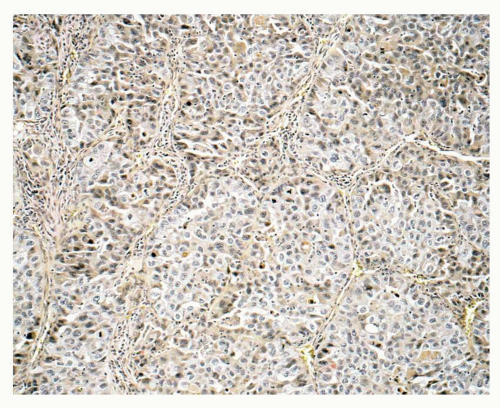 FIGURE 8-5 Medium-power image of mucicarmine stain of large cell carcinoma showing no cellular staining for mucin. |
LARGE CELL CARCINOMA, IMMUNOHISTOCHEMISTRY
The current WHO classification of non-small cell lung cancers is histology based and does not require immunostains for the diagnosis of adenocarcinoma, squamous cell carcinoma, and large cell carcinoma, and the use of immunostains to further characterize non-small cell carcinomas is controversial. Nonetheless, the institution of newer, molecular-based lung cancer therapies necessitates the differentiation of squamous cell carcinomas from other non-small cell carcinomas in order to avoid serious drug-related injuries. As such, the diagnosis of large cell carcinoma may decline in the future with the development of the use of immunostains to better characterize non-small cell lung cancers.7 Pardo et al.7 noted that the use of seven immunostains—TTF-1, CK7, CK19, p63, 34PE12, thrombomodulin, and CD44v6—dramatically reduced the number of
non-small cell lung cancers characterized as large cell carcinoma in a study of 101 lung cancer cases previously diagnosed as large cell carcinoma. Pardo et al.7 found that large cell carcinomas characteristically exhibit CK5/6 and CK14 immunonegativity, immunostains that are typically positive in squamous cell carcinomas; and MOC31 immunonegativity, an immunostain typically positive in adenocarcinomas. Large cell carcinomas also exhibited immunopositivity with EGFR, PDGFR-alpha, and c-kit.7 Pardo et al.7 reclassified over two thirds of the cases as adenocarcinomas or poorly differentiated squamous cell carcinomas (32.9% and 37.8%, respectively) based on immunopositivity with TTF-1, CK7, and CK19; and immunonegativity with p63 (adenocarcinomas) or immunopositivity with 34βE12, p63, thrombomodulin, and CD44v6 (poorly differentiated squamous cell carcinomas). Almost one fifth (19.5%) of large cell carcinomas were reclassified by the authors as adenosquamous carcinomas based on their exhibiting positivity with immunostains typically found to be positive in both adenocarcinoma and squamous cell carcinoma.7 Further studies will be of benefit in determining whether immunostain patterns in non-small cell lung cancers can successfully assist in categorizing poorly differentiated non-small cell carcinomas as adenocarcinomas or squamous cell carcinomas, thereby reducing the numbers of non-small cell lung cancers diagnosed as large cell carcinomas. The International Association for the Study of Lung Cancer suggests that in small biopsies containing non-small cell carcinoma without diagnostic features of adenocarcinoma or squamous cell carcinoma, and for which immunostains are noncontributory, the term “large cell carcinoma” not be used, and instead the term “non-small cell carcinoma, not otherwise specified” be used.
non-small cell lung cancers characterized as large cell carcinoma in a study of 101 lung cancer cases previously diagnosed as large cell carcinoma. Pardo et al.7 found that large cell carcinomas characteristically exhibit CK5/6 and CK14 immunonegativity, immunostains that are typically positive in squamous cell carcinomas; and MOC31 immunonegativity, an immunostain typically positive in adenocarcinomas. Large cell carcinomas also exhibited immunopositivity with EGFR, PDGFR-alpha, and c-kit.7 Pardo et al.7 reclassified over two thirds of the cases as adenocarcinomas or poorly differentiated squamous cell carcinomas (32.9% and 37.8%, respectively) based on immunopositivity with TTF-1, CK7, and CK19; and immunonegativity with p63 (adenocarcinomas) or immunopositivity with 34βE12, p63, thrombomodulin, and CD44v6 (poorly differentiated squamous cell carcinomas). Almost one fifth (19.5%) of large cell carcinomas were reclassified by the authors as adenosquamous carcinomas based on their exhibiting positivity with immunostains typically found to be positive in both adenocarcinoma and squamous cell carcinoma.7 Further studies will be of benefit in determining whether immunostain patterns in non-small cell lung cancers can successfully assist in categorizing poorly differentiated non-small cell carcinomas as adenocarcinomas or squamous cell carcinomas, thereby reducing the numbers of non-small cell lung cancers diagnosed as large cell carcinomas. The International Association for the Study of Lung Cancer suggests that in small biopsies containing non-small cell carcinoma without diagnostic features of adenocarcinoma or squamous cell carcinoma, and for which immunostains are noncontributory, the term “large cell carcinoma” not be used, and instead the term “non-small cell carcinoma, not otherwise specified” be used.
LARGE CELL CARCINOMA, DIFFERENTIAL DIAGNOSIS
Large cell carcinoma of the lung must be differentiated from poorly differentiated solid-type squamous cell carcinoma and solid-type adenocarcinoma primary in the lung, and from metastatic poorly differentiated carcinomas. Poorly differentiated squamous cell carcinomas contain foci of keratinization or intercellular bridges; and poorly differentiated adenocarcinomas contain foci of acinar formation or focal mucin (see Chapters 3, 6, and 17). Other differential diagnostic considerations include primary and metastatic lymphoma, sarcoma, and melanoma. Differential diagnoses of the variants of large cell carcinoma are discussed below.
LARGE CELL CARCINOMA, HISTIOGENESIS
Large cell carcinomas are believed to arise from a pleuripotent progenitor cell that is able to differentiate multidirectionally. As such, an in situ component is not characteristic of large cell carcinoma. The variants of large cell carcinoma, discussed below, most likely are a reflection of the tumor cells’ pleuripotentiality1
LARGE CELL CARCINOMA, VARIANTS
Clear cell carcinoma is a rare variant of large cell carcinoma that consists histologically of large polygonal cells with clear or foamy cytoplasm (Fig. 8-6). Areas of clear cell change maybe identi-fied in up to two thirds of non-small cell lung cancers, and clear cell variants of adenocarcinoma and squamous cell carcinoma exist and must be distinguished from clear cell carcinoma. Other differential diagnoses include clear cell (sugar) tumor of the lung, clear cell carcinoid tumor, and metastatic carcinomas that may have a prominent clear cell component such as renal cell carcinoma, salivary gland carcinomas, and thyroid carcinoma.1,2,4,8,9,10,11 and 12 Clear cell (sugar) tumor is generally immunopositive with HMB45 and immunonegative with cytokeratin, whereas clear cell carcinoma is typically HMB-45 immunonegative and cytokeratin positive.2
Large cell carcinoma with rhabdoid phenotype is another rare variant of large cell carcinoma that is an aggressive neoplasm. The diagnosis of large cell carcinoma with rhabdoid phenotype requires that at least 10% of the tumor be composed of rhabdoid tumor cells, which
are characterized by having large globular eosinophilic cytoplasmic inclusions, ultrastructurally shown to be composed of large intracytoplasmic paranuclear intermediate filaments (Fig. 8-7). The rhabdoid cells may be interspersed within the tumor, or arranged near the periphery of the tumor. Tumor cells generally grow in nests and sheets, and may exhibit an alveolar filling pattern. Nuclei show features of large cell carcinoma, including large, hyperchromatic nuclei and prominent nucleoli. The rhabdoid tumor cells are generally immunopositive with CK7, EMA, and vimentin; and immunonegative with CK20, TTF-1, muscle specific actin, and desmin. Some cases show immunopositivity with neuroendocrine marker, especially chromogranin. Differential diagnosis includes metastatic tumors with rhabdoid features.1,2,3,4,6,13
are characterized by having large globular eosinophilic cytoplasmic inclusions, ultrastructurally shown to be composed of large intracytoplasmic paranuclear intermediate filaments (Fig. 8-7). The rhabdoid cells may be interspersed within the tumor, or arranged near the periphery of the tumor. Tumor cells generally grow in nests and sheets, and may exhibit an alveolar filling pattern. Nuclei show features of large cell carcinoma, including large, hyperchromatic nuclei and prominent nucleoli. The rhabdoid tumor cells are generally immunopositive with CK7, EMA, and vimentin; and immunonegative with CK20, TTF-1, muscle specific actin, and desmin. Some cases show immunopositivity with neuroendocrine marker, especially chromogranin. Differential diagnosis includes metastatic tumors with rhabdoid features.1,2,3,4,6,13
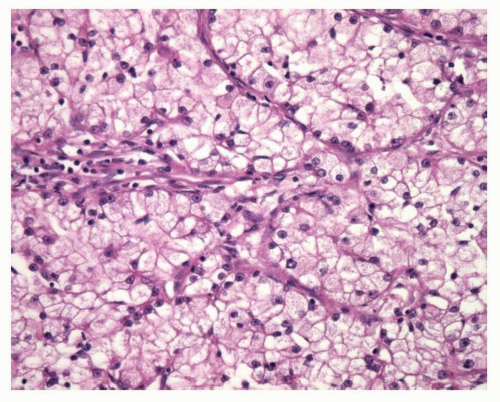 FIGURE 8-6 High-power image of clear cell carcinoma showing large polygonal cells with clear or foamy cytoplasm. In a case with these histologic features, care must be taken to exclude histologically similar metastatic tumors such as metastatic renal cell carcinoma. |
Lymphoepithelioma-like carcinoma is another rare variant of large cell carcinoma and is the only one that is not strongly related to smoking. Identified predominantly in Asians, often in middle-aged women, where it comprises up to 1% of lung tumors, lymphoepithelioma-like carcinoma is a variant of large cell carcinoma that is characterized histologically by syncytial sheets of large tumor cells with large vesicular nuclei, prominent nucleoli, numerous mitoses, and an associated marked inflammatory cell infiltrate made up of lymphocytes with admixed plasma cells and histiocytes, as well as interspersed eosinophils and neutrophils (Fig. 8-8). Amyloid may be identified occasionally. The inflammatory cell infiltrate is identified in metastatic
sites as well. Tumor often shows a pushing border. There is a strong association with Epstein-Barr virus in Asians, but the association is not strong in Western populations. Adenocarcinomatous or squamous cell differentiation is not found in lymphoepithelioma-like carcinomas. Information regarding prognosis is limited, but some patients may have a better prognosis than other non-small cell carcinoma patients. Differential diagnosis includes inflammatory pseudotumor, thymoma, melanoma, lymphoma, and metastatic nasopharyngeal carcinoma.1,2,3 and 4,14,15,16,17,18 and 19
sites as well. Tumor often shows a pushing border. There is a strong association with Epstein-Barr virus in Asians, but the association is not strong in Western populations. Adenocarcinomatous or squamous cell differentiation is not found in lymphoepithelioma-like carcinomas. Information regarding prognosis is limited, but some patients may have a better prognosis than other non-small cell carcinoma patients. Differential diagnosis includes inflammatory pseudotumor, thymoma, melanoma, lymphoma, and metastatic nasopharyngeal carcinoma.1,2,3 and 4,14,15,16,17,18 and 19
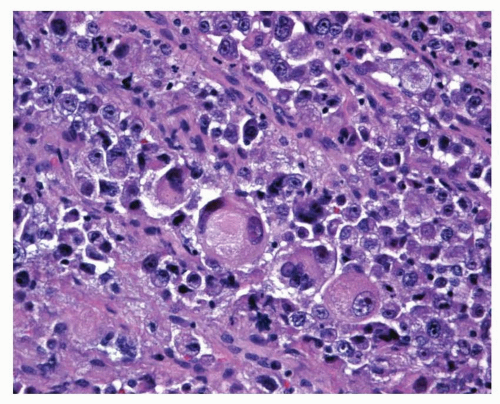 FIGURE 8-7 High-power image of large cell carcinoma with rhabdoid phenotype showing rhabdoid tumor cells, with large globular eosinophilic cytoplasmic inclusions and large hyperchromatic nuclei, some of which have prominent nucleoli. |
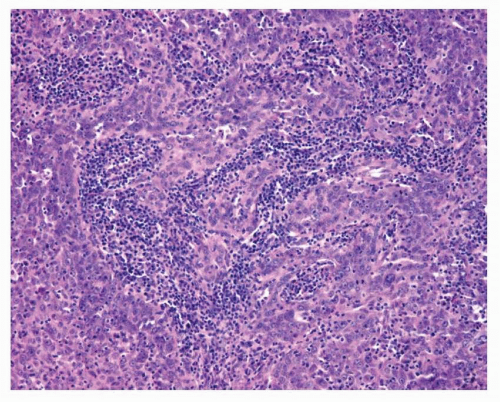 FIGURE 8-8 Medium-power image of lymphoepithelioma-like carcinoma showing syncytial sheets of large cell carcinoma tumor cells and an associated marked mixed chronic inflammatory cell infiltrate. |
LARGE CELL NEUROENDOCRINE CARCINOMA
Large cell neuroendocrine carcinoma of the lung is a variant of large cell carcinoma, the diagnosis of which requires that the large cell carcinoma show morphologic and ultrastructural or immunohistochemical features of neuroendocrine differentiation.1,2 and 3,20,21,22,23,24,25,26,27,28 and 29 Large cell neuroendocrine carcinoma is a relatively uncommon, smoking-related, aggressive lung cancer that makes up approximately 2% to 5% of all lung tumors.20,22,28,29 They frequently arise peripherally, but may arise centrally20,30 Radiographically, large cell neuroendocrine carcinomas are usually solid masses with irregular on CT scan, and cannot generally be distinguished from other non-small cell carcinomas or atypical carcinoid tumor. Central cavitation, as seen in squamous cell carcinomas, is infrequent. They may show associated emphysema, calcification, and pleural indentation.30,31 and 32
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


