Improving antimicrobial prescribing in the acute care setting is complex with multiple strategies that can be deployed by an antimicrobial stewardship program (ASP). How an ASP selects and implements interventions to improve antimicrobial prescribing is dependent on many factors. These factors include hospital size, hospital network status, training and background of ASP team members, time dedicated to stewardship activities, infectious diseases (ID) resources, pharmacist resources (especially ID pharmacists), information technology (IT) resources, and the culture and goals of the hospital. Each ASP is inherently unique and ideally has been molded to function in a specific hospital environment. As such, no “one size fits all” group of interventions, goals, policies, and daily work activities can be deployed with consistent results.
In this chapter, we highlight multiple antimicrobial stewardship (AS) interventions that have been shown to improve antimicrobial prescribing and the care of hospitalized patients. We do not recommend that a hospital implement all interventions immediately as this will cause substantial challenges and confusion. Rather, the selection of specific interventions and the degree in which they are implemented (ie, hospital-wide deployment vs targeting a specific unit) will be dependent on the maturity of the ASP and resources available. The selection of ASP interventions should be based on a clear understanding of the hospital needs and the goals of the ASP. Performing a needs assessment is an efficient and intentional method of identifying areas where an ASP should focus their efforts with new or expanded interventions. The Center for Disease Control and Prevention’s (CDC) Core Elements of Hospital Antibiotic Stewardship Programs Checklist is one example of a needs assessment that provides a framework to identify hospital ASP opportunities.1
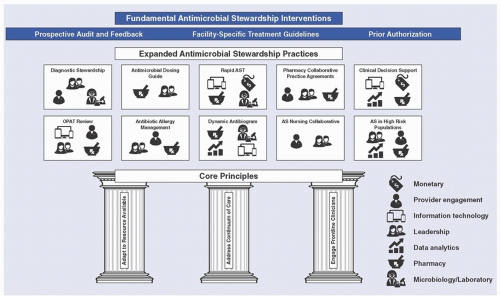
When selecting and implementing AS interventions, we recommend focusing on three key principles (Fig. 45-1). First, ASPs need to adapt and tailor AS interventions to the resources available. This adaptation will result in a more efficient and sustainable intervention. The interventions highlighted in this chapter have been successful in many hospitals; however, a deployment of the exact intervention in your hospital may not be similarly successful if the specific needs and hospital structure are not taken into consideration. AS interventions need to be tailored to the ASP team’s available time, the availability of ID consultation, the involvement of ID clinicians in ASP activities, electronic health record (EHR) capabilities, and hospital culture. Second, implement AS interventions across the continuum of inpatient care. Opportunities to improve antimicrobial prescribing occur throughout the course of patient’s admission. Using the “4 moments of antimicrobial decision making” as a framework,2 AS interventions can be implemented when (1) clinicians identify infections that will respond to antimicrobials and initiate empiric antimicrobial therapy (empiric selection), (2) proper diagnostic tests and cultures are performed and result (test selection and resulting), (3) stopping or narrowing empiric antimicrobials (de-escalation), and (4) determining the total duration of therapy of antimicrobials (duration of therapy). Ideally, an ASP will implement interventions targeting multiple “moments of antimicrobial decision making” to fully optimize prescribing. Third, engage frontline clinicians when selecting and/or implementing new AS interventions. When developing or implementing any new intervention, it is paramount to understand the attitudes, motivations, and intentions of those whose behavior is the target for change.3 Understanding the pressures and challenges faced by those on the receiving end of your intervention will allow the ASP to tailor interventions so they add value to the clinical team, target concerns of the frontline clinicians, and are perceived positively. In addition, understanding the local physical environment and schedules of your target audience will allow you to implement interventions that provide timely recommendations that are not disruptive to workflow. Engaging frontline clinicians in AS discussions and decisions will foster positive relationships and demonstrate your commitment to improving patient care.
FUNDAMENTAL INTERVENTIONS
As discussed above, ASPs should select and implement interventions that will target antimicrobial prescribing opportunities and goals that have been identified as highpriority targets. To most effectively address these opportunities, ASPs should prioritize AS interventions that have consistently shown improved antimicrobial prescribing and patient care in the medical literature. We have labeled these evidenced-based AS interventions as fundamental interventions. Fundamental interventions are backed by the strongest clinical evidence and are considered the foundation of an ASP.4 Fundamental interventions are adaptable to all hospitals regardless of size and stewardship staffing, target opportunities to improve prescribing across the continuum of care, and require the ASP to engage with frontline clinicians to build strong and lasting relationships. Each fundamental intervention can be expanded upon to enhance its reach and effectiveness based on resources available.
FIGURE 45-1 Fundamental antimicrobial stewardship interventions.
Develop and Implement Facility-Specific Treatment Guidelines
Facility-specific treatment guidelines for common ID syndromes are a fundamental intervention to direct antimicrobial therapy in hospitalized patients and can optimize empiric selection, de-escalation, and duration of therapy. Facility-specific treatment guidelines can be developed and adapted from national guidelines and modified based on local microbiology susceptibility data and formulary options. Lower respiratory tract infections (eg, pneumonia), urinary tract infections, and skin and soft tissue infections account for the majority of antibiotic use in hospitals.5 The development of treatment recommendations for these common syndromes should be a high priority for hospital-based ASPs.
Facility-specific treatment guidelines define antimicrobial prescribing appropriateness for clinicians at the local level. As such, the guidelines are best developed in multidisciplinary teams involving all relevant clinical stakeholders. For example, a community-acquired pneumonia guideline would be best developed with clinicians from pulmonary/intensive medicine, ID, emergency medicine, and hospital medicine. Involving clinical stakeholders from multiple disciplines will increase the likelihood of acceptance of recommendations. The appropriateness criteria defined in the guidelines can be used by the ASP when performing postprescription and prior authorization reviews (discussed below). In addition, well-defined treatment guidelines can be used as an audit tool when evaluating appropriate antimicrobial use during retrospective reviews.
Implementation and dissemination of local guidelines is often challenging in the acute care setting. Guidelines can be distributed and highlighted during formal and informal educational sessions, posted on the hospital intranet and in key patient care venues, and used in discussion during AS interactions. In addition, guidelines can be integrated into the clinician’s workflow by leveraging the EHR to incorporate recommendations into order sets and decision support tools. Lastly, guidelines can be kept relevant and useful to clinicians by undergoing annual review to incorporate changes in local data and updates in national guidelines. Providing current and clinically useful guidelines that have been developed with key stakeholders will improve the likelihood of clinician acceptance and clinical integration.
Prospective Audit and Feedback
Prospective audit and feedback is a method that allows the ASP to review current patient encounters and identify opportunities where antimicrobial management and patient care can be optimized. A prospective audit and feedback review is often initiated based on the antimicrobial prescribed (postprescription review [PPR]) or by clinical results obtained from the microbiology laboratory (microbiology and laboratory surveillance).
Postprescription Review PPR, also known as concurrent review, involves a member of the ASP performing a comprehensive review of a patient encounter after initiation of antimicrobials. This case review evaluates the current therapeutic plan looking for opportunities to improve antimicrobial prescribing and management of the patient. Recommendations are then relayed to the primary treatment team by the ASP and may include recommendations to de-escalate or escalate therapy, adjust duration of therapy, convert intravenous to oral formulations, and evaluate drug-drug interactions. When deployed effectively, PPR can result in reducing overall antibiotic use, cost, and length of stay. This review can be performed immediately after antimicrobials are prescribed or, more commonly, 2-48 hours after initiation. Waiting 2-48 hours provides the reviewer more clinical information (eg, laboratory results, microbiology results, clinical stability) upon which to base a recommendation. These reviews can occur Monday through Friday, 7 days a week, or at a different cadence dependent on AS resources. Given the vast differences in healthcare facilities, incorporating PPR into an ASP requires pragmatic consideration of each hospital’s needs and resources. For example, reviewing every patient on antimicrobials may be feasible at a small rural or community hospital, whereas the same approach at a large institution with several hundred patients would be impractical and time consuming. Because of this, developing an effective method of selecting and prioritizing specific antimicrobial therapies and/or combination therapies to review during PPR is vital. Table 45-1 provides examples of PPR targets that are often a focus of ASPs.
TABLE 45-1 Example Antibiotic Targets of Postprescription Review
Postprescription review targets
Example agents
Why review these agents?
Broad-spectrum, commonly used antibiotics
Cefepime, piperacillin-tazobactam, meropenem
Common drivers of antibiotic resistance and C difficile. Often used unnecessarily and are targets for de-escalation
Antibiotic agents used to treat drugresistant Gram-positive organisms
Daptomycin, vancomycin, linezolid, ceftaroline
Often used unnecessarily. Easily discontinued once cultures are negative
Identifying inappropriate use of highcost agents reduces unnecessary cost to the healthcare system and demonstrates financial incentive to expand stewardship resources
Preserving these agents for infections unable to be treated by conventional agents minimizes the risk of developing resistance and avoids the need for older, more toxic alternatives
Aligning the targets of PPR with the goals of the ASP will ensure that the reviewer’s time is used optimally. The specific approach to implementation of PPR (ie, agents selected and timing of review) can and should look differently at each hospital to account for the unique requirements and characteristics of each facility.
In addition to AS personnel time, other resources will contribute to the success, sustainability, and efficiency of PPR; some are arguably essential for any reasonable expectation of success in large hospitals. Prominent examples of crucial resources needed include IT and access to specialty trained AS personnel. Leveraging technology to aid in processing the vast amount of data required for PPR can reduce both the total number of patients requiring review as well as the time spent per patient.6,7 Many modern EHRs and clinical decision support systems (CDSS) can identify patients on specific antimicrobials for review by the ASP. See below for a more detailed discussion of CDSS. Lastly, given their training and expertise, ID-trained physicians and pharmacists are ideally suited to perform PPR and provide recommendations to the treating team. However, not all hospitals have access to ID-trained specialists to support the ASP and perform PPR. In these cases, hospitals can utilize interested physicians (often hospitalists) and general pharmacists to perform the reviews. Additional training for non-ID-trained clinicians can be obtained through the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, and the Society for Infectious Disease Pharmacists and Making a Difference in ID (MAD-ID). Appropriately trained staff can significantly impact the frequency and volume of reviews, the depth and complexity of the recommendations, and the confidence in which the recommendations are received.
Microbiology and Laboratory Surveillance-Focused Prospective Audit and Feedback Prospective audit and feedback can also be initiated from clinical results obtained from the microbiology or clinical laboratory. Just like PPR, laboratory-initiated interventions should be prioritized based on the critical nature of the test result and institution-specific needs that have been previously identified. For example, ASPs with limited personnel or resources should focus on the review of sterile site cultures (eg, blood) that have a high risk of morbidity and mortality if treated inappropriately. In contrast, well-staffed ASPs may review all positive cultures to evaluate for opportunities to de-escalate therapy. Additional results that can trigger a review include positive Clostridioides difficile tests, multidrug-resistant pathogens identified in any culture type, positive microbiology cultures in patients not on antibiotic therapy, and infection-related biomarkers, serologies (eg, HIV), or viral studies. The review of positive C difficile tests has been shown to be a high-yield stewardship intervention.8
Molecular rapid diagnostic tests (mRDTs) have emerged as a key technology to decrease the time to identification and antimicrobial susceptibility of infecting pathogens. These tests, when used appropriately, can decrease the time to effective antimicrobial therapy, improve timely antibiotic de-escalation, and decrease length of stay in patients with bloodstream infections. Importantly, the clinical impact of mRDTs is most pronounced when the results are reviewed and acted upon by the ASP in real time as part of their prospective audit and review program.9,10 The successful implementation of mRDTs is dependent on creating workflows to support AS review of mRDTs results and effectively communicating recommendations to frontline clinicians. Incorporating mRDTs results into the ASP workflow should be a high priority in hospitals that utilize this technology.
Prior Authorization
Another fundamental practice of AS is prior authorization, otherwise known as antimicrobial restrictions. Prior authorization requires certain antimicrobial agents to be approved prior to initiating therapy. This process typically requires the prescriber to contact a member of the ASP to obtain authorization, which is typically based on policies jointly established by the ASP and the Pharmacy and Therapeutics committee of the hospital. The most common reasons a hospital or health system will restrict antimicrobial agents include cost of the drug, narrow therapeutic index requiring specialized knowledge in dosing and monitoring, and broad-spectrum agents that should only be used to treat specific highly resistant pathogens.
Prior authorization has an advantage of allowing direct control over specific agents and has been shown to decrease designated antimicrobial use, decrease overall medication cost, and improve antibiotic resistance among Gram-negative pathogens.11 In addition, a mature prior authorization program can be used to manage difficulties with drug acquisition and drug shortages by adding antimicrobials to the list of restricted drugs as needed. Instituting a prior authorization program requires the ASP to consider many operational and logistic challenges. Who will receive the request for the restricted antimicrobial—a pharmacist, internal medicine resident, ID fellow, or an ID attending? Having clear, local appropriate use criteria for restricted agents can allow non-ID-trained clinicians to participate in the prior authorization program and ensure consistency of recommendations.12 What happens if the requesting physician is insistent on using the denied antimicrobial agent? Who will mediate the disagreement? Will restrictions be in place 24 hours a day, 7 days a week, and on holidays? Many facilities do not have the capacity to provide around-the-clock reviews, requiring some facilities to modify the process to allow initiation without approval on nights/weekends with a follow-up review during normal business hours. Since prompt antimicrobial therapy is extremely important in the critically ill, can the clinician receive a first-time dose if the ASP is not available to review the request in order to not delay care? These questions will need to be addressed before starting a prior authorization program. Lastly, ASPs with heavy prior authorization requirements can have potential disadvantages as well. The most significant disadvantage may be the impedance it places on provider autonomy, which has been shown to create a negative perception of AS and damage the rapport necessary for effective collaboration.13 Actively managing these concerns and ensuring prior authorization requests are used as collaborative and educational opportunities will instill a team-based approach to better patient care.
Postprescription Review vs Prior Authorization
PPR and prior authorization have long been identified as the two pillars of AS interventions. Two studies have compared these two interventions directly. In a large academic center, PPR and prior authorization were compared in a crossover trial of adult inpatients.14 PPR was found to result in decreased antibiotic days of therapy, decreased length of therapy, and improved antibiotic appropriateness at day 3 of therapy. The second trial compared PPR with a modified prior authorization (first dose did not require approval) in a non-randomized crossover design in four community hospitals in North Carolina.15 Again, PPR review was found to reduce antibiotic use compared to historical controls while the restrictive strategy did not. Additionally, PPR resulted in the AS team having more contact with treating clinicians than did prior authorization. Many experts suggest that these interventions are synergistic and both should be priorities for implementation. Hospitals can use local data, predefined goals, and time allocation to determine how much of each intervention to blend into their ASP.
EXPANDED PRACTICES
In contrast to the fundamental practices, expanded practices have not yet become standard AS practices for all hospitals. Many of the expanded practices described below have a significant body of evidence to support their practice, but incorporating these interventions into ASPs is often limited by the resources required and specialized knowledge needed. Once hospitals have implemented the fundamental practices of AS, the expanded practices can be evaluated and implemented based on need, expertise, and time available.
Diagnostic Stewardship
Microbiologic testing is a cornerstone of appropriate ID care. Rapid and accurate diagnosis of infection is critical to ensure appropriate antimicrobial therapy initiation and optimal subsequent management. In addition, appropriate diagnostic testing often identifies infecting pathogens and allows clinicians to optimize and narrow antimicrobial therapy. However, when diagnostic tests (eg, standard bacterial cultures or pathogen-specific molecular tests) are used inappropriately and identify an organism(s) that represents colonization or contamination, an infection may be inadvertently diagnosed. Patients that receive a diagnosis of an infection when an infection is not present are often treated with unnecessary antibiotics and have a delay in identifying the correct diagnosis that is causing their symptoms.16 In addition, some of the nationally reported healthcareassociated infections (HAIs) are identified entirely by a laboratory test or culture. Inappropriate testing, resulting in over-diagnosis of HAIs, can therefore increase a hospital’s publicly reported infection rate with resultant downstream consequences.17
TABLE 45-2 Examples of Diagnostic Stewardship Interventions That Can Be Led by Antimicrobial Stewardship Programs
Test
Why a diagnostic stewardship intervention is needed?
Possible antibiotic stewardship program intervention
Expected result
Urine culture
Urine cultures are commonly performed and often detect asymptomatic bacteriuria, which results in inappropriate antibiotic therapy
While performing prospective audit and feedback, identify patients with urine cultures without symptoms referable to the urinary tract and ensure they do not receive antibiotics
Diarrhea is a common symptom in hospitalized patients. Many patients are colonized with C difficile. Overtesting patients for C difficile leads to inappropriate diagnosis and treatment with further disruption of the gastrointestinal microbiome
Educational campaign on appropriate testing
Electronic health record (EHR) alerts to discourage C difficile testing when laxatives were recently received20
Microbiology laboratory interventions to reject samples of formed stool
Decreased treatment of patients with C difficile colonization.
Decreased healthcareassociated C difficile cases
Molecular syndromic respiratory panels
Multiplex PCR-based respiratory pathogen panels often contain over 10 targets. These panels are often costly and detect respiratory viruses that have no treatment available. Large panels have not been shown to improve outcomes.21 Pathogenspecific respiratory viral tests are available (eg, influenza) at a fraction of the cost and provide actionable data
Educational campaign on appropriate testing
EHR-based tools to discourage testing and promote pathogen-specific tests
Decreased cost for the patient and healthcare system
Only gold members can continue reading. Log In or Register to continue
 Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
 Healthcare-Associated Infections Related to the Use of Intravascular Devices
Healthcare-Associated Infections Related to the Use of Intravascular Devices
 MDRO Infections: Gram-Positive Organisms (Including Methicillin-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococcus)
MDRO Infections: Gram-Positive Organisms (Including Methicillin-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococcus)
 Epidemiology and Prevention of Healthcare-Associated Infections Related to Animals in the Hospital
Epidemiology and Prevention of Healthcare-Associated Infections Related to Animals in the Hospital



