Fig. 7.1
The contraceptive triangle
The science and art in contraceptive counseling and care consists in providing a perfect fit between these three interacting groups of variables.
7.2.1 Method Variables
Objective characteristics derived from experimental data: pharmacodynamic properties, pharmacokinetics, way of application, interactions with other drugs, and metabolizing enzymes
Probability characteristics derived from statistical data: Pearl index (Life Table Analysis), health risks, health benefits, and side effects
7.2.2 Patient Variables
Subjective characteristics: individual preferences, values, and family planning objectives
Biopsychosocial profile:
Biomedical characteristics: diseases and drugs (personal history), age, weight, blood pressure, and genetic outfit
Psychosocial characteristics: education and professional situation
7.2.3 Situation Variables
Phase of life
Relationship characteristics
7.3 Contraceptive Counseling and Care as an Interactive, Structured Process
A structured process is best suited to provide the optimal interaction of these variables. This process follows basic bioethical principles [26]:
Respect of autonomy. This means in contraceptive counseling that the objectives and values of the patient (client) are respected.
Nonmaleficence. Do not harm means that she or he is effectively protected against unwanted pregnancies and that health risks and negative side effects are minimized.
Beneficence. This principle means that the health and well-being of the patient is promoted and cared for.
Justice. All patients (clients) should have the same access to contraceptive information and care.
7.3.1 Step 1: Assess the Woman’s Expectations and Preferences (Respect of Autonomy)
In the first step the professional should assess the individual woman’s expectations, objectives, and preferences. This corresponds to the ethical principle of respect of autonomy.
Women may have very different objectives and values. The following are some examples:
Objectives
Absolute need to prevent pregnancy in the context of life situation
Pregnancy not absolutely unwanted but not now
Spacing pregnancies
Family planning fulfilled, no more children
Etc.
Values and needs
Natural method
Easy to use
Independent of partner
Involvement of partner
Safety high priority
Fear of health risks
Etc.
The information obtained in this part of the interview is important for step 4a in the decision-making process.
7.3.2 Step 2: Assess the Woman’s Biopsychosocial Profile and Life Situation (Objective Patient and Situation Variables)
We differentiate between findings (objective facts), risks (probabilities), and conditions (elements of quality of life) [22–25].
7.3.2.1 Biomedical Dimension
Findings (age, BMI, blood pressure)
Risks (cardiovascular risks, neoplastic risks, metabolic risks, STI risks, bone risks)
Conditions (hyperandrogenemic signs, dysmenorrhea, mastalgia, PMS, PMDD, etc.)
These data are assessed through a careful clinical history and examination. Findings and risks are important for step 4 (see below) in the structured process. Information about preexisting physical complaints and elements of quality of life are significant for step 5 (see below).
7.3.2.2 Psychological Dimension
Findings (depression, anxiety, drug abuse)
Risks (behavioral risks, STI risks)
Conditions (somatoform disorder, sexual dysfunction)
The psychosocial history, the open interview, and the assessment of present complaints provide this information. Of special importance are the behavioral characteristics and preexisting emotional problems for step 4 and step 5 (see below).
7.3.2.3 Social Dimension
Findings (socioeconomic status, education)
Risks (cultural restrictions, dependence, migration)
Conditions (stress, relationship issues)
Especially the sociocultural background and the present relationship characteristics are important elements of this part of the clinical interview, and they have an impact on step 4 (see below).
7.3.3 Step 3: Educate Women About Methods with Understandable Risk/Benefit Information Based on EBM Results (Method Variables) (Beneficence)
This step should empower women and help them to make informed choices. It is thus part of beneficence duty of the professional.
Women should be informed about the methods in a way that responds to two demands:
(a)
The information should be based on the latest scientific evidence.
(b)
The information should be given in didactic, understandable way and adapted to the individual needs of the patient.
The first request is quite easily feasible; the second is much more difficult. Some general guidelines of information giving are as follows:
Elicit preexisting knowledge and questions.
Provide clear and simple information:
Give information in small units.
Encourage questions.
Summarize and repeat.
Elicit the understanding and the meaning given by the patient.
The issues and questions concerning the information exchange are as follows.
7.3.3.1 How Effective is Method x, y, and z to Prevent an Unwanted Pregnancy?
This question can be answered by a visual aid showing the efficiency of the methods if used by 100 women for 1 year.
The typical information to be given refers to the lowest expected percentage of women with a pregnancy during the first year of use [6, 15].
Highly effective methods:
Combination pill 0.1 %, progestin only 0.5 %, IUD copper T380A 0.6 %, levonorgestrel IUD 0.1 %, implant 0.1 %, injectable 0.3 %, female sterilization 0.2 %, and male sterilization 0.1 %
Medium effective methods:
Male condom 3 %, ovulation method 3 %, symptothermal 2 %, and post ovulation 1 %
Methods with low effectiveness:
Withdrawal 4 %, spermicides 6 %, diaphragm and spermicides 6 %, calendar 9 %, and cervical cap (parous women 20 %, nulliparous 9 %)
7.3.3.2 How Much is the Effectiveness Dependent on Proper Use?
The discussion of this issue points to the discrepancy between theoretical and typical Pearl index and allows a classification with respect to the necessary compliance and discipline [6, 15].
Methods with high demand on compliance:
Combination pill (lowest expected rate 0.1 % versus typical use rate 5–7.6 %)
Condom (lowest expected 3 % versus typical use rate 10–14 %)
Methods with low demand on compliance:
IUDs (lowest expected rate 0.1–0.6 % versus typical use rate 0.1–0.8 %)
Implants (lowest expected rate 0.2 % versus typical use rate 0.2 %)
7.3.3.3 What are the Health Risks of the Method?
This is a crucial part of the information exchange process. It is important to give a risk background and to describe risks in absolute numbers or give some points of reference [15, 23, 27].
High risk: between >1 and 1 in 100
For example: Gastrointestinal side effects of antibiotics 10 in 100; risk of pregnancy while using spermicides 6 in 100
Moderate risk: between 1 in 100 and 1 in 1,000
For example: Death due to smoking 10 cigarettes/day: 5 in 1,000
Having a baby with Down syndrome at age 35 years: 5 in 1,000
Low risk: between 1 in 1,000 and 1 in 10,000
For example: Venous thromboembolism attributable to COC: 3 to 6 in 10,000
Death due to car accident: 12 in 10,000
Diagnosis of breast cancer under 45 years possibly attributable to current OC use: 8 in 10,000
Very low risk: between 1:10,000 and 1:100,000
For example: Death due to soccer playing: 4 in 100,000
Risk of death from all causes in OC users: 1 in 100,000
After the general understanding of risk, the patient should be informed about the typical risks or the methods [15, 24, 27–34].
Combined OCs:
Venous thromboembolic disease, myocardial infarction, and stroke – very low absolute risk (1 case in 10,000 users down to 3 in 100,000 users)
Breast cancer and cervical neoplasia – very low absolute risk
Progestogen only:
No or very low health risk
IUDs copper:
Perforation, PID, and ectopic pregnancy – low to very low risk
Levonorgestrel IUS:
Perforation, PID, and ectopic pregnancy – low to very low risk
7.3.3.4 What are the Factors that Influence the Health Risks (Increase or Decrease)?
This information helps the patient to understand her personal nonmodifiable and modifiable risks. She can learn about the impact of a healthy lifestyle on her individual risk during the use of different contraceptives [15, 27, 35, 36].
Reduce cardiovascular risks by controlling weight, exercising, stopping smoking, and lowering cholesterol.
Reduce risk of STI, PID, and CIN by using condom and avoiding sex with “risky” partners or under risk conditions (alcohol, drugs, etc.).
7.3.3.5 What are the Possible Noncontraceptive Health Benefits of the Method?
It is important to give not only information about risks but also about possible noncontraceptive health benefits of the methods.
For example, condoms diminish considerably the risk to acquire a sexually transmitted disease (for HIV with consistent use at about 97 %, against HSV highly effective, against HPV not very effective) [37].
For example, OC benefits are less endometrial cancer, less ovarian cancer, fewer ectopic pregnancies, more regular menses (less flow, less dysmenorrheal, less anemia), less salpingitis, increased bone density, probably less endometriosis, possibly less benign breast disease, possibly less rheumatoid arthritis, possibly protection against atherosclerosis, possibly fewer fibroids, and possibly fewer ovarian cysts [15, 38].
For example, levonorgestrel IUD reduces blood loss in hypermenorrhea, possibly diminishes fibroma size, and may protect against PID [34].
7.3.3.6 What are the Most Frequent Possible Negative and Positive Side Effects Having an Impact on the Quality of Life?
It is important to comment on possible negative and positive side effects at the same time. Many of the effects observed by the patient are very individual and cannot be predicted. Mentioning possible negative effects is important to avoid unnecessary anxiety, disappointment, and insecurity.
Related posts:
 Management of Adolescent Hyperandrogenism
Management of Adolescent Hyperandrogenism
 Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Supplementation with DHEA in Poor Responder Patients
Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Supplementation with DHEA in Poor Responder Patients
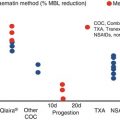 Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
 Low Malignant Potential Tumors
Low Malignant Potential Tumors
 Disorders of the Menstrual Cycle During Adolescence
Disorders of the Menstrual Cycle During Adolescence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


