Chapter 60 Hemophilia A and B
Table 60-1 Factor VIII Mutant Genotype and Inhibitor Risk in Previously Untreated Hemophilia A Patients
| Multidomain deletions | ≈75% |
| Light chain nonsense mutns | 30%-40% |
| Intron 22 inversion | 20%-25% |
| Single domain deletions | 15%-25% |
| Small non-A run insertions/deltns | 15%-20% |
| Heavy chain nonsense mutns | 10%-20% |
| Factor VIII missense mutns | <10% |
| Small A run insertions/deltns | <5% |
| Splicing mutns | <5% |
Table 60-2 Methods of Factor VIII Measurement
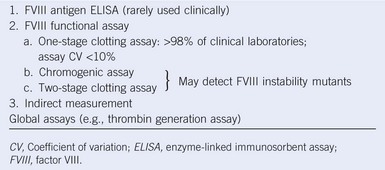 |




