Autologous transplant involves first harvesting peripheral blood stem cells from the patient before treatment with high-dose chemotherapy and/or radiotherapy, then infusion of the cells after treatment to reconstitute the marrow. The most common hematologic malignancies treated with autotransplant are multiple myeloma and lymphoma.
Allogeneic transplant is performed for hematologic malignancies when the marrow itself is diseased—stem cells are obtained from peripheral blood, marrow, or cord blood from a related or unrelated donor with matching HLA type. Manipulation of the stem cell product may be done to reduce the risk of graft vs. host disease (GVHD), such as CD34 selection or T-cell depletion. The most common indications for allogeneic transplants include acute leukemia, myelodysplastic syndrome, aplastic anemia, or congenital immunodeficiency disorders.
Newer indications, including autoimmune disorders, such as lupus and rheumatoid arthritis, and sickle cell anemia.
An expanded armamentarium of immunosuppressive agents including novel immunotherapy agents (e.g., rituximab and ofatumumab—chimeric and human monoclonal antibody against CD20; alemtuzumab—monoclonal antibody against CD52; infliximab—monoclonal antibody against TNF-α; daclizumab—monoclonal antibody to interleukin-2 (IL-2) receptor; and so on).
More accurate HLA typing.
Discovery of the role of natural killer (NK) cell typing (12).
Use of peripheral blood and umbilical cord blood as stem cell sources. The HLA matching criteria for cord blood transplant (CBT) are less stringent (13,14), making CBT
a critical treatment option for patients without suitable donors.
Appreciation of the benefits of graft-vs.-leukemia. This has led to reduced intensity conditioning (RIC) regimens, sometimes referred to as “nonmyeloablative” or “mini” transplant. RIC can be given to an older population as well as to outpatients (15,16,17,18,19). RIC regimens are now used in 40% of allogeneic HSCTs performed.
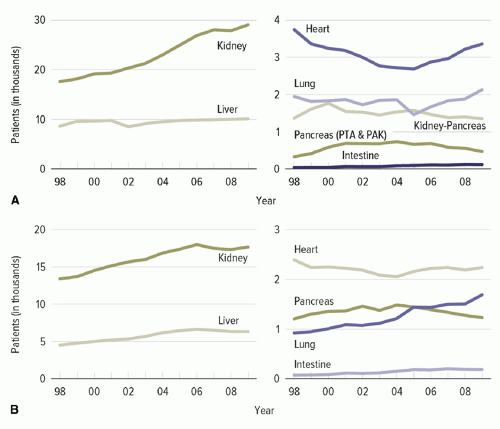 Figure 45.1. (A) Patients added to the waiting list during the year. (B) Transplants performed during the year. The trends in solid organ transplant in the last decade (1998 to 2008) by organ type. With permission from Organ Procurement and Transplantation Network (OPTN) and Scientific Registry of Transplant Recipients (SRTR). OPTN / SRTR 2010 Annual Data Report. Rockville, MD: Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation; 2011. http://www.srtr.org/annual_reports/2010/. Accessed October 8, 2012. |
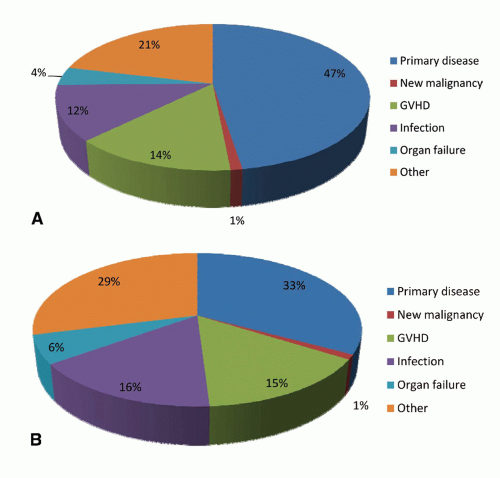 Figure 45.2. The causes of death after allogeneic HSCT performed in the years 2008 (A) and 2009 (B). Adapted from Pasquini MC, Wang Z. Current use and outcome of hematopoietic stem cell transplantation: CIBMTR summary slides, 2011. http://www.cibmtr.org, with permission. |
The presence of anatomic abnormalities related to surgery or disruption of the mucocutaneous barrier by indwelling devices.
Environmental factors, including exposure to organisms in the community or the hospital.
The patient’s net state of immunosuppression.
Those related to surgery itself, such as biliary abnormalities in liver transplant and ureterovesical reflux after renal transplant. Additional examples include complications at the time of the transplant that result in the creation of devitalized tissue, fluid collections, and/or ongoing urine or bile leaks, and posttransplant complications, such as organ ischemia. Unless such abnormalities are promptly eliminated, secondary infection is inevitable (21).
Perioperative breaches of mucocutaneous surfaces by vascular access devices, endotracheal tubes, drainage devices, or urinary catheters are associated with secondary infection. Removal of these devices is indicated as early as possible. The incidence of device-related infection is related to the nature of the transplant (small bowel = liver > lung = pancreas > heart > kidney), the complexity of the surgery, and the duration of time that “devices” compromise the integrity of the skin. In addition, hematomas are iron-rich and therefore may promote the growth of Listeria, the Zygomycetes, and other microbes (22,23,24).
come to transplant such as chronic hepatitis, biliary cirrhosis, or inflammatory lung disease. The intensity and duration of such immunosuppressive therapy administered has a direct impact on the net state of immune compromise. Third, active infection with one or more immunomodulating viruses (e.g., cytomegalovirus [CMV], Epstein—Barr virus [EBV], human herpesvirus-6, hepatitis viruses B [HBV] or C [HCV], or HIV) may add to the net state of suppression. Finally, conditions common to the immunocompromised host such as damage to the mucocutaneous surfaces of the body, neutropenia, or metabolic abnormalities such as protein—calorie malnutrition, uremia, or hyperglycemia all may additionally compromise immune function.
TABLE 45.1 Induction and Maintenance Immunosuppressive Agents Used in Solid Organ Transplant | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
occurrence of GVHD and its treatment with pharmacologic immunosuppression, as well as the immunomodulating infections listed above determine the pace of immune reconstitution and susceptibility to infection.
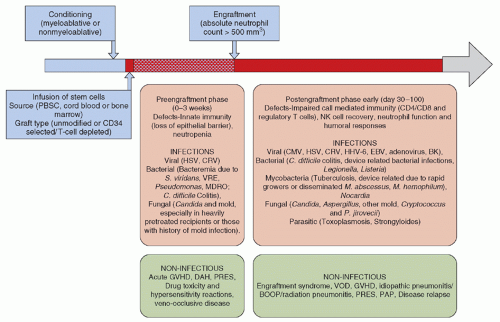 Figure 45.3. The time course of allogeneic stem cell transplant and associated infectious and non-infectious complications. |
(114,115). Rituximab leads to a decline in neutralizing antibodies that maintain virologic control in patients with chronic HBV infection and those with isolated core HBV antibody positivity. Reactivation is known to occur as long as 1 year after the last dose of rituximab, and screening for HBV infection with serologic testing for hepatitis B surface antigen and hepatitis B core antibody and antiviral prophylaxis are routinely recommended (116,117,118,119,120,121). Rituximab use has also been associated with persistent and relapsing infection with Babesia microti (122). The treatment of babesiosis in this setting can be particularly challenging, requiring long-term antibiotics and risk of emergence of resistance. Other infections with significant association with rituximab administration include enterovirus 71 meningoencephalitis (123), CMV (124,125,126), and Polyomavirus infections (JC and BK) (127,128,129,130,131).
(141,142,143,144); postprocedure pneumonia (lung) (145,146); mediastinitis, sternal infections, or pneumonia (heart). Indwelling devices, including urinary or intravascular catheters, further increase the risk of infection for all SOT recipients.
Symptom screening—All admissions to the floor should be screened for respiratory symptoms and daily symptom assessment performed for all admitted patients as well as for all healthcare workers who work on the floor, including those, such as food and nutrition and radiology workers, who spend only limited time on the floor. Patients with respiratory symptoms should not be admitted to transplant ward and symptomatic healthcare workers furloughed until no symptoms and negative repeat test for influenza. Visitors should be limited and appropriately screened for symptoms daily.
If sustained transmission occurs 48 hours after implementing these measures, all nonessential admissions should be postponed. In addition, the number of healthcare workers entering the patients’ room must be limited and floating staff discontinued. A designated triage area should be created at the entrance to the ward for screening of visitors and nursing leadership designate staff for daily healthcare worker screening.
Isolation precautions—Infected persons should be placed under droplet precautions (i.e., single room, mask, gowns, and gloves) and susceptible patients should be placed under reverse or protective precautions (i.e., single room, mask, and gloves).
Antiviral treatment should be started on all infected persons irrespective of the duration of symptoms in an attempt to reduce the period and intensity of viral shedding.
Prophylaxis should be offered to all susceptible persons regardless of their vaccination status. M2 inhibitors should be avoided unless the virus is known to be susceptible. Asymptomatic persons receiving prophylaxis do not have any visitation or work restrictions.
Vaccination should be offered and made readily accessible for all susceptible individuals.
Patient and staff education should be emphasized (particularly hand hygiene, cough etiquette, symptom screening, and vaccination).
Viral testing for all symptomatic persons should be done promptly.
transplantation Ad Hoc Disease Transmission Advisory Committee set interim guidelines advising against recovering lungs and intestine from donors known to be infected with novel H1N1 virus and lungs from donors with seasonal influenza (213).
and fomites. DFA and viral culture have poor to moderate sensitivity (50%) for the detection of PIV, especially PIV4. PCR greatly improves the detection of these viruses from respiratory samples (44,172,223).
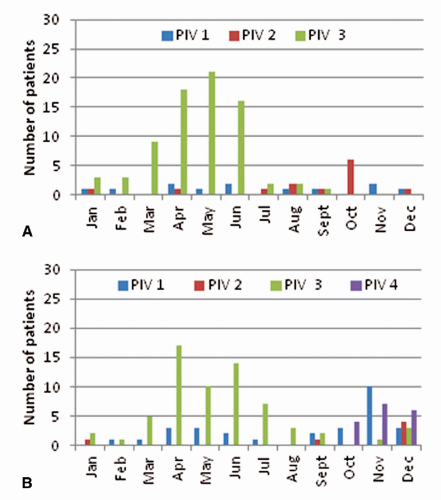 Figure 45.4. The seasonal distribution of parainfluenza viruses by subtype in the years 2010 (A) and 2011 (B). |
Related posts:
 Epidemiology of Healthcare-Associated Infections
Epidemiologic Methods for Investigating Infections in the Healthcare Setting
Economic Evaluation of Healthcare-Associated Infections and Infection-Control and Antimicrobial-Stewardship Interventions
The Intensive Care Unit, Part B: Antibiotic Resistance and Prevention of CVC-BSIs, Catheter-Associated Urinary Tract Infections, and C. difficile
Nosocomial Tuberculosis
The Importance of Infection Control in Controlling Antimicrobial-Resistant Organisms
Epidemiology of Healthcare-Associated Infections
Epidemiologic Methods for Investigating Infections in the Healthcare Setting
Economic Evaluation of Healthcare-Associated Infections and Infection-Control and Antimicrobial-Stewardship Interventions
The Intensive Care Unit, Part B: Antibiotic Resistance and Prevention of CVC-BSIs, Catheter-Associated Urinary Tract Infections, and C. difficile
Nosocomial Tuberculosis
The Importance of Infection Control in Controlling Antimicrobial-Resistant Organisms
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


