Group 1A: Example 2.2
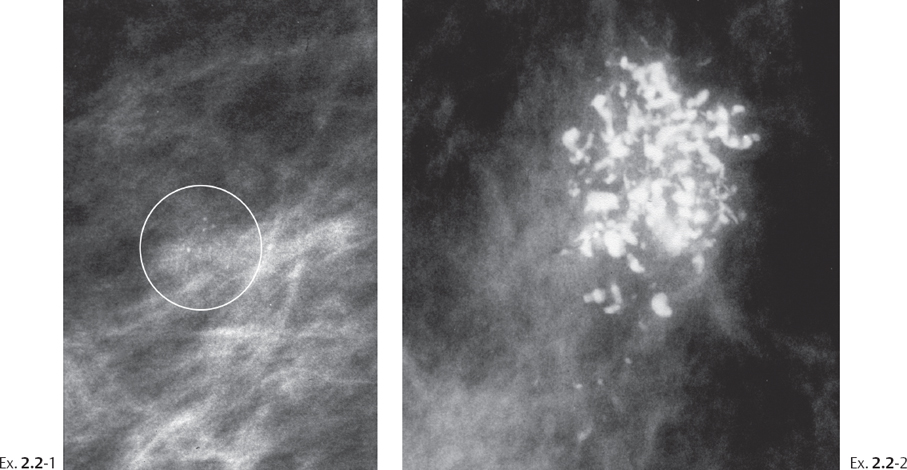
A 70-year-old asymptomatic woman, screening examination. The faint cluster of crushed stone-like calcifications was not perceived. At her next screening examination 18 months later she was still asymptomatic and was called back for further assessment of the cluster of calcifications.
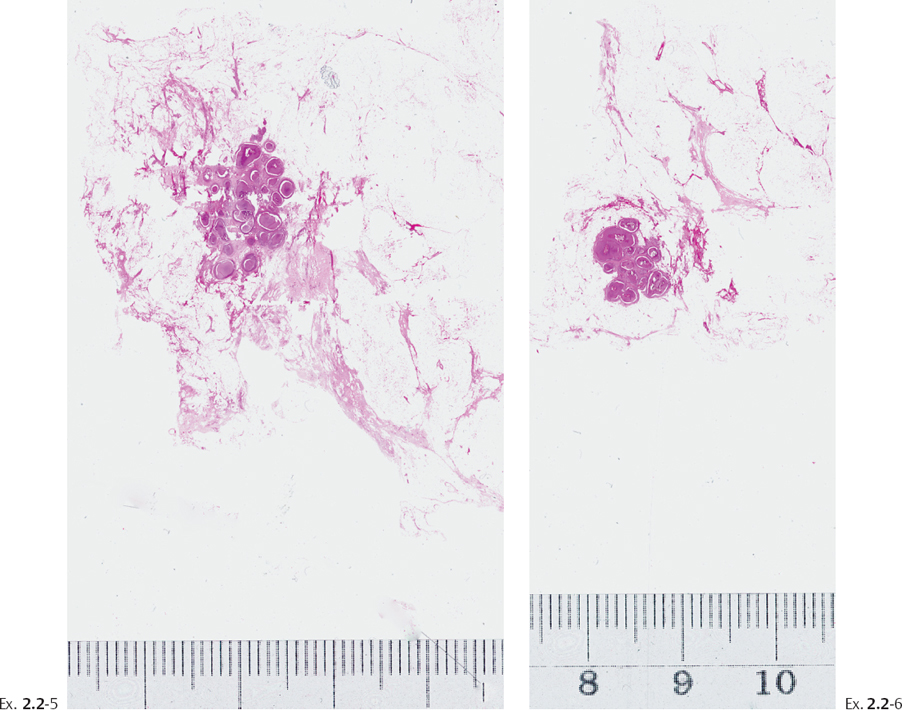
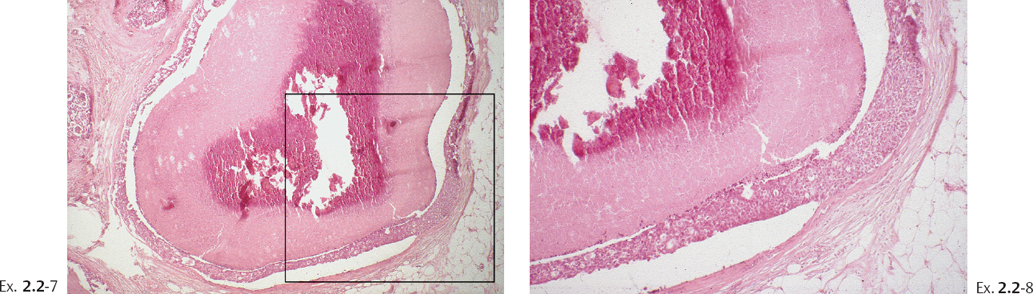
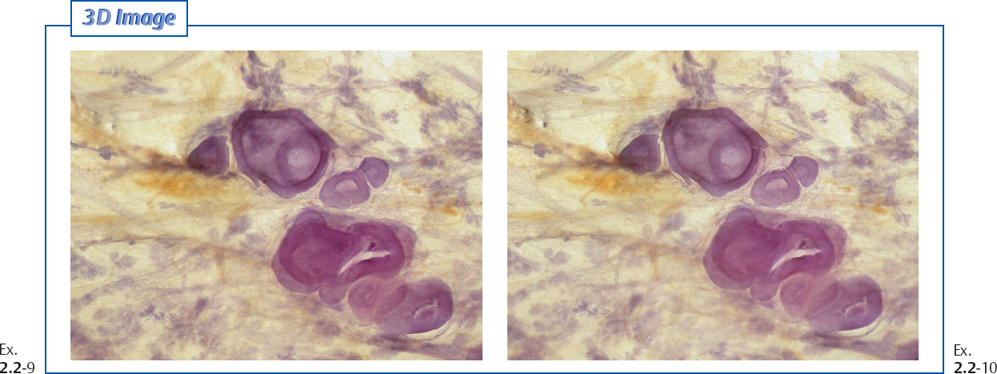
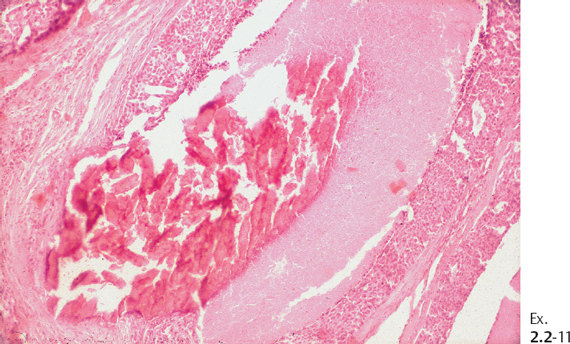
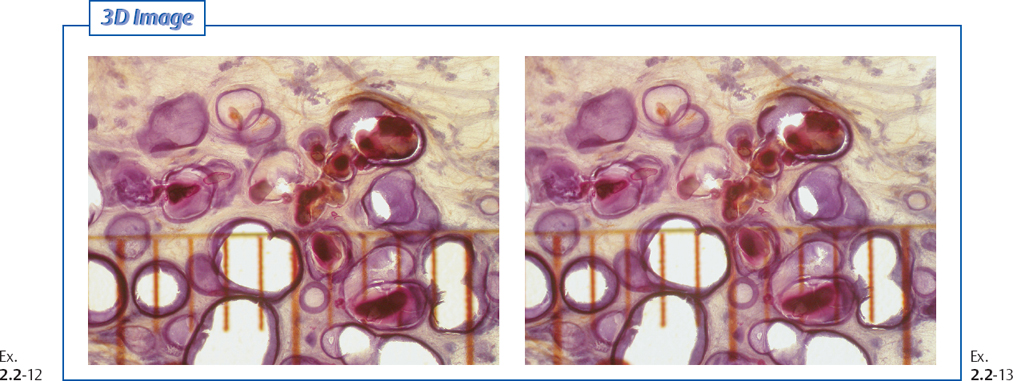
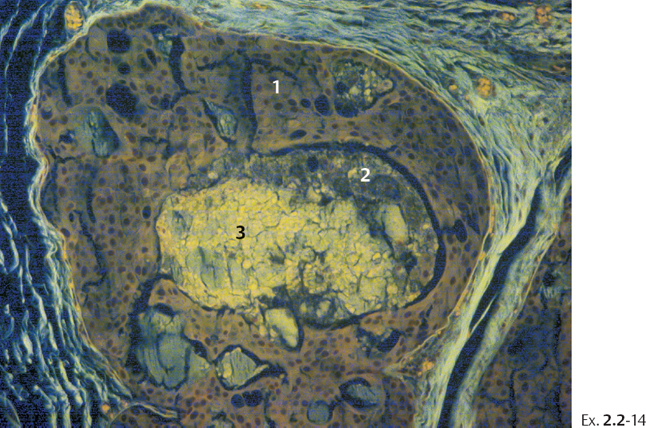
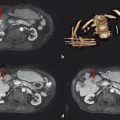
Histological diagnosis: 18 mm ⊠ 11 mm ⊠ 8 mm Grade 3 in-situ carcinoma with solid and cribriform cell architecture, containing multiple foci of microinvasion.
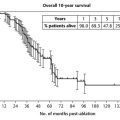
Treatment and follow-up: Sector resection was performed. No postoperative radiotherapy or other adjuvant treatment was given. The patient had no evidence of breast cancer at the most recent follow-up, 12 years after operation.
Comment
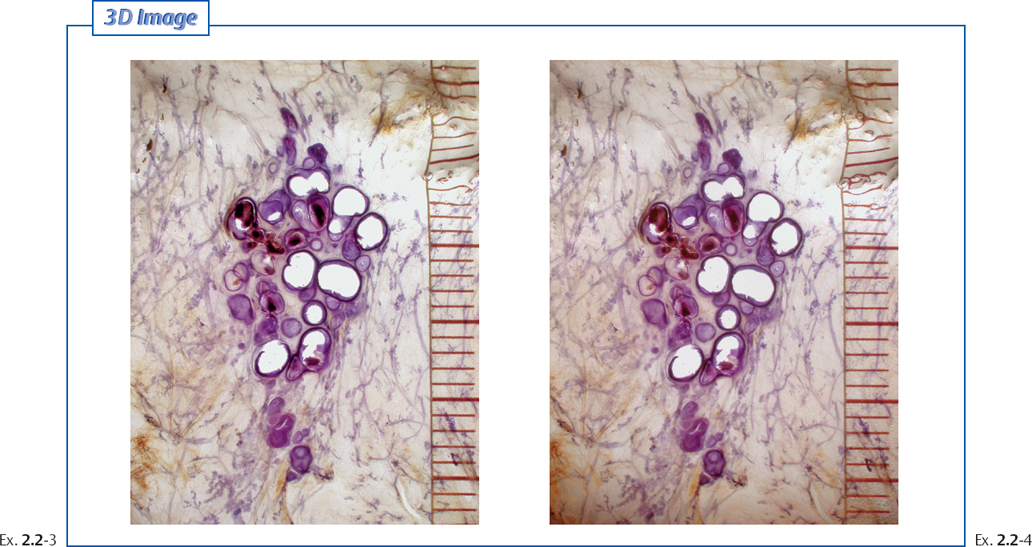
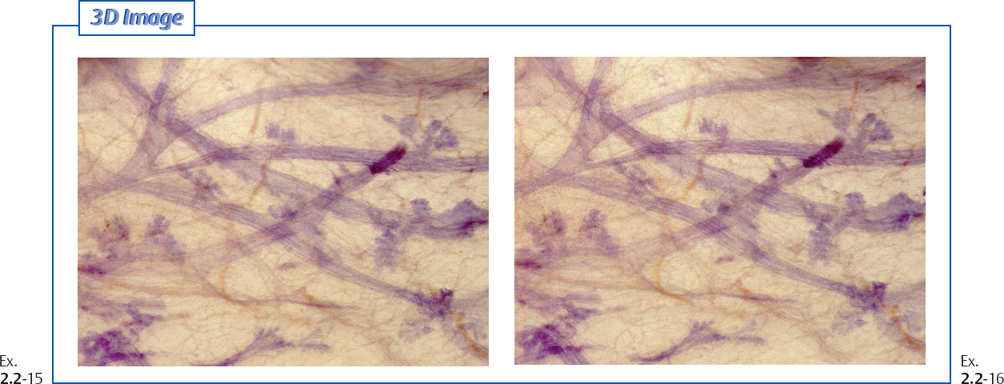
The large-section histological image and the subgross 3D images clearly show that the disease was limited to a single, extremely distended TDLU. The malignant cells were confined to I the acini of the lobule and no ductal involvement was found. These observations are at odds with the conventional term “ductal” carcinoma in situ. Sefton R. Wellings and his co-workers pointed out that pathologists, viewing traditional, small histological sections, might have mistaken the extremely distended acini for ducts.1 The fact that the disease is restricted to a single, isolated TDLU should be a justification for less radical treatment, such as surgical excision alone without adjunctive therapy.
Related posts:
 Group 1A: Example 2.1
Group 1A: Example 2.1
 Classification of Crushed Stone-like Calcifications Produced by Malignant Processes
Classification of Crushed Stone-like Calcifications Produced by Malignant Processes
 Overview of the Diagnostic and Management Problems Encountered When Malignant Type Calcifications Are Detected on the Mammogram
Overview of the Diagnostic and Management Problems Encountered When Malignant Type Calcifications Are Detected on the Mammogram
 14 Urothelial Cancer and Transitional Cell Cancer
14 Urothelial Cancer and Transitional Cell Cancer
 7 Colorectal Hepatic Metastatic Disease: Ablation
7 Colorectal Hepatic Metastatic Disease: Ablation
 13 Emerging Technologies in Interventional Oncology
13 Emerging Technologies in Interventional Oncology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


