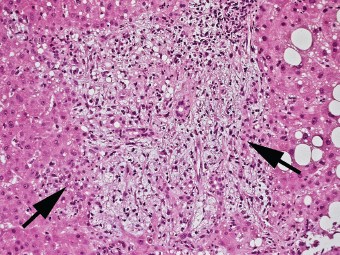
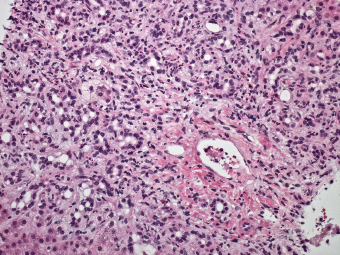
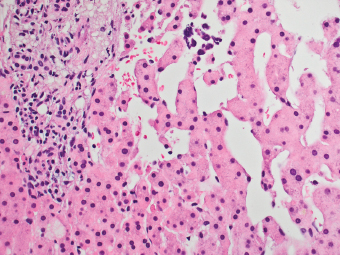
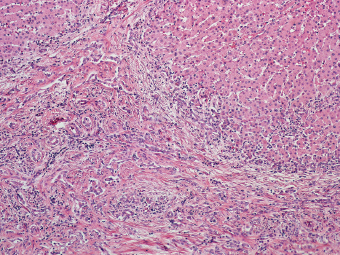
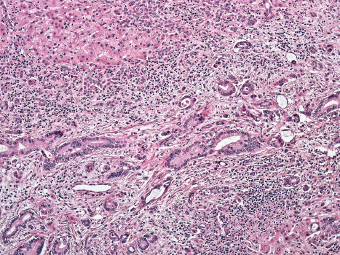
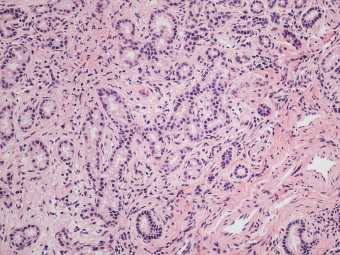
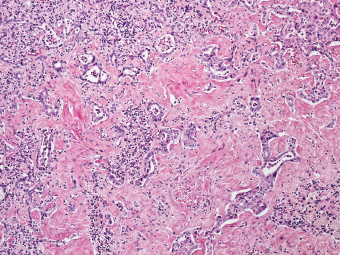
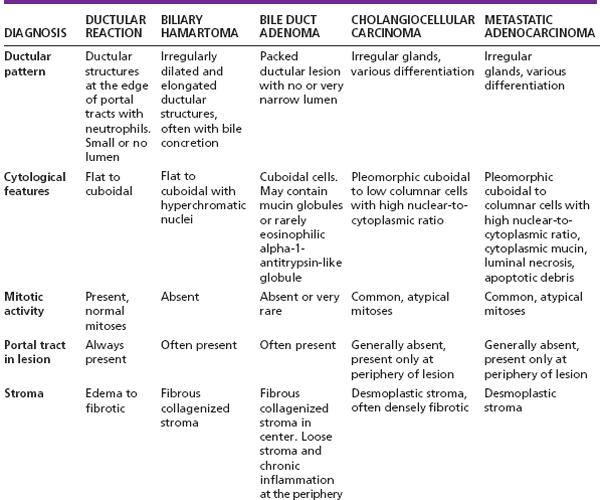
8 Biologic Evolution and Treatment Biologic Evolution and Treatment Biologic Evolution and Treatment Glandular neoplastic mimics of the liver are commonly encountered during frozen section examination. Coupled with inherent frozen section artifact and reactive atypia, these lesions can be difficult to interpret in a rushed circumstance. The basic information that the operators are requesting is whether the lesion is a benign lesion or malignant neoplasm; and perhaps after the distinction between benign and malignant has been reached, a more definitive diagnosis of the type of lesion or resemblance to a known primary lesion can be rendered although this may not be necessary in most instances. Glandular neoplastic mimics in general can be divided into two types of lesions, localized and diffuse lesions. Localized lesions include biliary hamartoma and bile duct adenoma; whereas diffuse lesions include ductular reaction and congenital hepatic fibrosis. Ductular reaction is benign proliferation of ductular structures at the margin of the portal tracts. Ductular structures may arise from proliferation of preexisting cholangiocytes, progenitor cells (local and/or circulating cells probably bone marrow derived), or biliary metaplasia of hepatocytes (443). Synonyms include typical or atypical ductular proliferation, proliferating bile ductules, and biliary piecemeal necrosis. Ductular reactions occur in various conditions including neoplastic and neoplastic mimic diseases, such as large bile duct obstruction secondary to gallstones, cholangiocarcinoma, pancreatic tumor, mass-associated changes (primary or metastatic tumors, abscess) due to localized duct obstruction, significant interface hepatitis, and response to submassive hepatic necrosis. Unless a space-occupying lesion is detected in the vicinity, ductular reactions produce no discernible mass; therefore, ductular reactions will not be suspected radiologically. Ductular reaction occurs at the edge of the portal tracts. The portal tracts are typically expanded and occasionally edematous, with a pale watery appearance to the fibrous connective tissue. The ductular structures contain small or no discernible lumen, lying roughly parallel to the limiting plate, and can be irregular in clusters or tangles (Figure 8.1). Active ductular reaction is always accompanied by neutrophils (Figure 8.2). Bile extravasation and lakes are often seen due to rupture of these structures, particularly in the cases of large bile duct obstruction. Ductular reaction is often part of tumor-associated changes in the adjacent parenchyma caused by localized bile duct obstruction (Figure 8.3). In addition to ductular reaction, chronic inflammation and focal sinusoidal dilatation and congestion without zonal predilection are also present (444). The adjacent liver cell plates are compressed and distorted with atrophy of the hepatocytes. These changes are the result of local obstruction of blood and bile flow by an expanding primary or metastatic lesion. In chronic biliary diseases or chronic large duct obstruction, ductular reaction is more diffusely spread in the portal tracts and fibrous bands, accompanied by lymphocytic infiltrate and fewer neutrophils. The stroma becomes more densely fibrotic and less edematous (Figure 8.4). FIGURE 8.1 Large bile duct obstruction causes ductular reaction at the edge of portal tracts (arrows), accompanied by neutrophils. The portal tract is edematous with a pale watery appearance. FIGURE 8.2 Exuberant ductular reaction expands the portal tract and is accompanied by neutrophilic infiltrate. FIGURE 8.3 Ductular reaction may be part of tumor-associated changes in adjacent parenchyma due to localized bile duct obstruction. Sinusoidal dilatation is often also observed. It should lead to rebiopsy. FIGURE 8.4 In biliary cirrhosis, ductular reaction is diffusely embedded in the portal tracts and fibrous bands. Edematous stroma with ductular reaction is seen only around the cirrhotic nodule resulting in a “halo” appearance. In submassive or massive hepatic necrosis, ductular reaction extends diffusely into the lobules, reflecting progenitor cell activity in the absence of adequate hepatocellular regeneration. The portal tracts become closer to one another and condensation of reticulin framework is observed due to the extensive loss of the hepatocytes. The differential diagnoses of ductular reaction include bile duct adenoma, biliary hamartoma, cholangiocarcinoma, cholangiolocarcinoma, and metastatic adenocarcinomas. Marked atypia in an otherwise benign ductular reaction is often observed in frozen section specimens submitted to rule out primary or metastatic tumors. Portal edema accompanying neutrophilic infiltrate, periportal location of the ductular structures, and the presence of normal portal tract structures (original bile duct, hepatic artery, and portal vein) are helpful in the diagnosis of ductular reaction. Well-differentiated cholangiocarcinoma and cholangiolocarcinoma are often difficult to distinguish from ductular reaction due to the lack of significant cytological atypia, necrosis, or mitotic activity (Figures 8.5 and 8.6). Well-differentiated cholangiocarcinoma is composed of small neoplastic ductular structures in the background of dense desmoplastic stroma (Figure 8.7). The advancing front of the neoplasm is hypercellular and the center of the neoplasm is usually hypoor acellular. Immunohistochemical stains can be helpful if diagnostic confusion with ductular reaction occurs (see Table 8.1). FIGURE 8.5 Well-differentiated cholangiocarcinoma composed of atypical glands involving the portal tract. Some of the neoplastic glands can be similar to ductular reaction at the edge of the portal tract. FIGURE 8.6 Cholangiolocarcinoma composed of neoplastic ductular proliferation “cholangioles.” FIGURE 8.7 Atypical neoplastic ductular structures of cholangiocarcinoma are embedded within dense collagenized desmoplastic stroma.
Glandular Neoplastic Mimics of the Liver
 PSEUDOCARCINOMATOUS LOCALIZED HEPATIC ATROPHY
PSEUDOCARCINOMATOUS LOCALIZED HEPATIC ATROPHY
INTRODUCTION
DUCTULAR REACTION
 CLINICAL AND IMAGING FEATURES
CLINICAL AND IMAGING FEATURES
 PATHOLOGICAL FEATURES
PATHOLOGICAL FEATURES
 DIFFERENTIAL DIAGNOSES
DIFFERENTIAL DIAGNOSES






Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


