CHAPTER 29 Giardiasis
Clinical Manifestations
Clinical symptoms of Giardia infection range from asymptomatic cyst passage to acute, self-limited diarrhea, to prolonged diarrheal disease.1–3 Asymptomatic infection is common. Symptoms of acute illness include watery diarrhea with abdominal pain; stools may be foul-smelling with accompanying flatulence, abdominal distension, and poor appetite. A small proportion of patients will develop a prolonged diarrheal syndrome with intermittent diarrhea, abdominal and epigastric discomfort exacerbated by eating, malaise, fatigue, and occasional headache, often leading to weight loss (a distinguishing feature) and anemia. Lactose intolerance is common (20–40% of cases), may persist for weeks after infection, and may be mistaken for relapse or reinfection.4 Giardia has been implicated in growth failure in children in the developing world who are chronically infected or frequently reinfected. Catch-up growth has been shown to occur when Giardia is eliminated.
The disease is transmitted by ingestion of cysts. Onset of symptoms occurs 1–2 weeks after cyst ingestion, though the period of time to detection of cysts in the stool may be longer than the incubation period. The disease is communicable for as long as cyst passage occurs (may be as long as 6 months).1
Individuals with humoral immunodeficiencies are at increased risk of chronic disease if infected.
Etiology
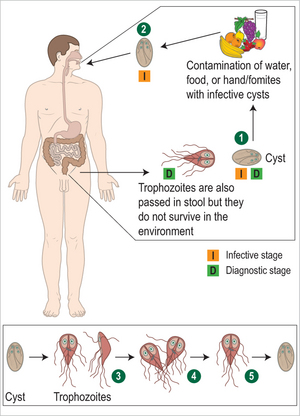
Giardia is a flagellate protozoan. The two stages in the life cycle are the free living trophozoite form, and the infectious form, the cyst. Acquisition of disease is by ingestion of as few as 10–25 cysts, occurring most frequently by drinking contaminated water, but also by person-to-person transmission. Under the influence of gastric acid, excystation releases trophozoites which colonize and multiply in the upper small bowel and biliary tract (Fig. 29.1).2
Epidemiology
Giardiasis occurs worldwide, in both temperate and tropical climates. Giardia is one of the first parasites to infect children in the developing world; prevalence rates may be as high as 15–20% in children under 10 years of age. Over 60% of children may be infected at some point during childhood.1 In the US, it is the most commonly identified intestinal parasite, with prevalence rates as high as 16% in some areas. Outbreaks have been associated with contamination of water supplies, exposure to water contaminated by animal feces containing cysts infectious for humans, and person-to-person transmission in settings such as childcare centers. Food-borne transmission also occurs. Exposure to infected feces may also occur during sexual contact.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


