Successful management of the neck is a prerequisite for the cure of most head and neck squamous cell carcinomas (HNSCC). Tumor spread to the regional nodes signals the transformation of the primary tumor to a more malignant phenotype with the ability to not only invade lymphatics but also spread hematogenously. Indeed, the clinical involvement of the regional node decreases the chance for cure by at least one-half.1 Even in a clinically negative neck, surgical data have demonstrated high rates of occult nodal involvement for the majority of head and neck primary sites. Usually, such regional spread occurs in a predictable, progressive pattern depending on the mucosal site of origin, local richness of lymphatics, proximity to midline, and tumor stage. Thus, in a clinically negative neck, the first echelon nodes and levels of potentially involved nodal stations are evaluated and risk of involvement assessed before a decision is rendered regarding selective management. For clinically node-positive patients, more comprehensive, intensive treatment is required that addresses the greater tumor burden and larger areas of potential spread. How the neck is managed usually follows the manner in which the primary site is addressed. Single modality therapy, either surgery or radiation, is used to manage early stage primary tumors and regional lymphatics at risk for harboring occult disease, whereas multidisciplinary approaches are required for advanced primary tumors. Although surgery was traditionally considered the mainstay of treatment of the primary site and neck, decades of randomized trials have established radiation therapy as an effective alternative. In that regard, advances in organ preservation therapies have resulted from the integration of concurrent chemotherapy with radiation2,3,4,5,6 altered fractionated radiation therapy,7,8,9,10 introduction of new chemotherapeutic/biologic agents,11 use of induction chemotherapy,12,13 better understanding of the role of functional imaging improved treatment techniques such as intensity-modulated radiation therapy (IMRT)14,15 as well as advances in molecular profiling, especially with regard to the human papilloma virus and epidermal growth factor receptor. Recent improvements in transoral robotic techniques have renewed primary surgical approaches for multiple sites (oropharynx and hypopharynx). In this regard, a neck dissection is usually performed in a staged manner, which has emphasized risk-adapted adjuvant treatment based on pathologic factors.
The purpose of this chapter will be to discuss the role of surgery and radiation therapy in the elective, adjuvant, and definitive management of the neck. Additionally, this chapter will discuss the use of imaging to assess oncologic response and to discuss evolving concepts which may better tailor treatment of regional disease. The management of regional metastatic disease from nasopharyngeal cancer will be discussed in a separate chapter.
CERVICAL LYMPH NODE LEVELS
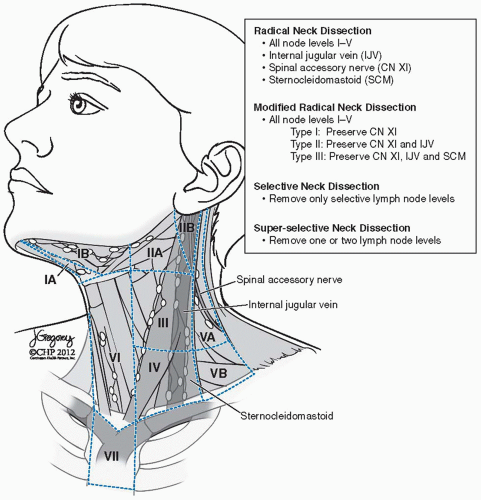
The Committee for Head and Neck Surgery and Oncology of the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) first published the guidelines for anatomic boundaries of the various cervical levels in 1991,16 which were modified and updated in 2002.17 These guidelines were all based on the original level designations that were created at Memorial Sloan Kettering Cancer Center to refer to the particular topographical location on the neck under which a consistent pattern of lymph nodes existed (Fig. 14-1).
NECK STAGING
It is clear that metastases to cervical lymph nodes has a profound impact on the prognosis of a patient. The current staging system is based on a consensus between the European UICC and American Joint Cancer Committees. This system utilizes the clinical features of nodal size, number, and laterality. It does not integrate imaging features suggestive of extranodal extension, which is well known to adversely affect prognosis. Table 14.1 describes the N staging.
FIGURE 14-1. Nodal delineation for the electively treated node-negative and node-positive neck. On the left, are nodal stations delineated in a node-negative neck. On the right, are target delineation of level II nodal level up to the skull base in a node-positive neck. On the left, is shown the target delineation of level II in an electively treated neck. Note the differences in the superior margin allows substantial sparing of the parotid gland. RP, retropharygeal node; ICA, internal carotid artery; JV, jugular vein; PG, parotid gland; PB of JGD, posterior belly of the jugulodigastric muscle; BP, brachial plexus. See Table 14.10 for boundaries of nodal stations. (See color insert.)
Patients staged as Nx have regional lymph nodes that cannot be assessed. NO patients have no identifiable regional nodal metastasis. N1 patients have a single nodal metastasis, ipsilateral to the primary tumor site, and <3 cm in greatest dimension.
Patients staged as N2a have a metastasis to a single ipsilateral node, which is >3 cm but <6 cm in greatest dimension. Patients staged as N2b have metastasis to multiple ipsilateral lymph nodes and none are >6 cm in greatest dimension. Patients staged as N2c have metastatic disease in bilateral or contralateral lymph nodes; none are >6 cm in greatest dimension. Patients staged as N3 disease have a lymph node or conglomerate of lymph nodes >6 cm in dimension.
TABLE 14.1 Cervical Lymph Node Staging System
AJCC 1976
AJCC 1983
UICC-AJCC 1987-2002
NO
No involved node
No involved node
No involved node
N1
Single ipsilateral node <3 cm
Single ipsilateral <3 cm
Single ipsilateral <3 cm
N2
1. Single ipsilateral >3 cm, <6 node cm
2. Multiple ipsilateral <6 cm
1. Single ipsilateral >3 cm, <6 cm
2. Multiple ipsilateral >3 cm, <6 cm
1. Single ipsilateral >3 cm, <6 cm
2. Multiple ipsilateral <6 cm
3. Bilateral or contralateral <6 cm
N3
1. Ipsilateral node(s)>6 cm
2. Bilateral
3. Contralateral only
Node >6 cm
NECK DISSECTION TERMINOLOGY
Radical neck dissection: Radical neck dissection involves removal of lymph node levels I to V, including the submandibular gland, tail of the parotid gland, sternocleidomastoid muscle, internal jugular vein, and spinal accessory nerve (Fig. 14-2).
Modified radical neck dissection (MRND): MRND involves removal of lymph nodes from levels I to V (as in the radical neck dissection) but with preservation of at least one of the nonlymphatic structures (i.e., sternocleidomastoid muscle, spinal accessory nerve, and/or internal jugular vein).Modifications to the radical neck dissection include the following: (a) Type I: The spinal accessory nerve is preserved; (b) Type II: The spinal accessory nerve and the internal jugular vein are preserved; (c) Type III: The spinal accessory nerve, the internal jugular vein, and the sernocleidomastoid muscle are preserved.
FIGURE 14-2. Removal of lymph node levels I to V.
Extended radical neck dissection: Extended radical neck dissection refers to removal of additional lymph node levels or groups and/or nonlymphatic structures (i.e., muscle, blood vessels, nerves) not normally removed with a radical neck dissection. Examples of additional lymph node groups include superior mediastinal, parapharyngeal, retropharyngeal, periparotid, postauricular, suboccipital, and buccinator. Examples of other nonlympahtic structures are the external carotid artery, hypoglossal and vagus nerves, and other neural, osseous, cutaneous, muscular, or vascular structures that are potentially involved with tumor.
Selective neck dissection (SND): SND refers to preservation of one or more lymph node levels and sparing all vital structures (sernocleidomastoid muscle, internal jugular vein, spinal accessory nerve). There are several variations of the SND, which have been given specific names (i.e., lateral, supraomohyoid, extended supraomohyoid, posterior, and central) (Fig. 14-3A-C).
Super selective neck dissection: Super selective neck dissection involves complete removal of all fibrofatty tissue contents, including lymph nodes, along the defined boundaries of one or two contiguous neck levels.18
The super selective neck dissection has been pioneered by Robbins et al. who have utilized the super selective neck dissection in patients with advanced head and neck cancer that have been treated with primary chemoradiation and have residual pathologic lymphadenopathy limited to a single lymph node level.18,19 It is believed that by minimizing the surgical field, soft tissue fibrosis is reduced and its impact on swallowing, mastication, and range of motion of the neck are minimized.
THE EVOLUTION OF THE NECK DISSECTION
Surgeons of the early 19th century were aware that cancers of the head and neck metastasized to cervical lymph nodes; they often regarded this as a sign of incurability.20 It was believed that the cervical metastases needed to be removed with the primary tumor, in order for the patient to have any chance of survival. In 1888, Jawdynski published the first description of an en bloc neck dissection, which was later popularized by George W. Crile, who published a systematic approach to the neck dissection in 1906.21 In this procedure, all lymphatic tissue between the superficial and deep cervical fascial layers of the lateral neck were removed en bloc, including the sternocleidomastoid muscle, internal jugular vein, tail of the parotid gland, submandibular gland, and spinal accessory nerve.
In 1951, Hayes Martin and colleagues published their experience with 1,450 cases of neck dissections.22 This paper helped to define the technique, as well as gain acceptance within the surgical community. In 1952, Suarez published his modifications of the classical radical neck dissection, which he called the “functional neck dissection.” The goal of the functional neck dissection was to reduce morbidity while preserving the oncologic efficacy of the classic radical neck dissection. The modifications made by Suarez were preservation of the sternocleidomastoid muscle, internal jugular vein, omohyoid muscle, and, whenever possible, the spinal accessory nerve. Bocca and colleagues went on to popularize the selective removal of cervical lymphatics with preservation of vital structures (i.e., sternocleidomastoid muscle, spinal accessory nerve, internal jugular vein).23 Preserving these structures allows for maximization of control of the regional disease with minimization of the morbidity associated with a radical neck dissection (chronic neck and shoulder pain, cosmetic deformity, facial edema, etc.).
FIGURE 14-3. Selective neck dissection. A: Selective removal of lymph node levels II, II, and IV. B: Illustration of selective remova of lymph node levels II, II, and IV. C: Neck after selective removal of lymph node levels II, II, and IV. (See color insert for Part B).
At this point, surgeons had become adept at systematically removing cervical lymphatics, but it was not until 1972 when Robert Lindberg first recognized patterns of cervical metastases in correlation with the primary tumor location.24 This publication revealed that there were clear and predictable patterns of spread in the cervical lymphatics from each subsite within the upper aerodigestive tract. This observation that the patterns of cervical nodal disease are dictated by the location of the primary tumor has enabled surgeons to selectively remove nodal basins at risk for metastases based on the primary site of disease. This newfound knowledge opened the doors for preservation of low-risk nodal basins, thus decreasing patient morbidity. In the 1980s, Ballantyne from M. D. Anderson Cancer Center became one of the initial proponents of the SND. In 1988, Byers et al. described the patterns of nodal metastasis among 428 patients with HNSCC.25 In 1990, Shah reported the progression of metastatic disease in the neck in a consecutive series of 1,081 patients with primary tumors of the oral cavity, the oropharynx, the hypopharynx, and the larynx.26 The SND is now routinely used as a staging procedure to determine the presence or lack of occult metastases (which can help in the decision to apply adjuvant radiation therapy). More recently, the SND has been utilized in N+ necks as well as in postchemoradiation planned neck dissections. The use of the SND in clinically positive necks has been gaining widespread acceptance in recent years.
CURRENT PHILOSOPHY FOR LATERAL COMPARTMENT NECK DISSECTIONS
The contemporary approach to removing cervical lymphatics has evolved from the highly morbid radical neck dissection to the much less morbid yet effective SND. Although the pendulum has shifted to a much less aggressive extirpation of lymphatic and nonlymphatic tissues, the radical neck dissection still remains the gold standard by which all modifications to the neck dissection must be compared. The current philosophy of ablative surgeons can be distilled down to a few simple goals. The first is the removal of all clinically positive lymph nodes and all involved nonlymphatic structures. The second goal is to preserve all nonlymphatic structures, which are not diseased, to optimize functional outcomes. The third goal is removal of all lymph node levels, which are at high risk for harboring metastatic disease. With these simple but clear goals, ablative surgeons are now more thoughtful in their extirpation.
CENTRAL COMPARTMENT NECK DISSECTION
The central compartment (level VI) is important to address when managing patients with thyroid cancer and those tumors with subglottic extension. The boundaries for the central compartment of the neck (level VI) are the carotid arteries laterally, the hyoid bone superiorly, and suprasternal notch inferiorly. The inferior border of a central compartment neck dissection is located below the sternal notch at the level of the innominate artery and brachiocephalic vein (level VII). A comprehensive central compartment neck dissection incorporates level VI and level VII lymph nodes. These lymph node echelons are most commonly associated with metastases from thyroid cancer. In papillary thyroid cancer, the incidence of central compartment metastases has been reported between 21 % and 60%.27,28 Lymph node metastases in patients with papillary thyroid cancer are associated with a higher recurrence rate.29 There is evidence that patients 45 years of age or older with regional nodal metastases have a higher mortality rate.30 There is also evidence that patients with clinically evident nodal disease who undergo lymphadenectomy may have a reduced rate of recurrence and mortality.29,31,32 Therefore, there is general agreement that clinically involved lymph nodes should be removed and comprehensive central compartment neck dissection should be performed in this situation.
A prophylactic central compartment neck dissection is defined as a level VI lymph node dissection in patients with no evidence of lymph node metastases on preoperative physical examination or imaging. A prophylactic central compartment dissection remains controversial because occult metastatic disease within the central compartment of patients with papillary thyroid cancer have been reported to range between 31% and 62% and rarely become clinically relevant.28,33,34 In most series, the rate of recurrence in the central neck for patients with a papillary thyroid cancer >1 cm that were clinically node negative and were treated with total thyroidectomy without a central compartment neck dissection is 2 % to 3 %.33,34,35,36 Currently, there has been no proven benefit for a prophylactic central compartment neck dissection.
ROLE OF CAROTID ARTERY RESECTION IN NECK DISSECTION
Direct invasion or encasement of the carotid artery may occur in cases of advanced HNSCC. Resection of the carotid artery remains controversial because of the significant morbidity and mortality which may be associated with it. The prognosis for these patients is poor with the 1-year disease-free survival (DFS) ranging from 0% to 44%.37,38 The surgical alternatives consist of peeling the tumor off the carotid artery which may be palliative or curative, carotid resection without revascularization, and carotid resection with vascular bypass grafting. Since complete tumor removal is the most important prognostic factor in head and neck surgery, peeling the tumor of the carotid artery is not considered an oncologically sound resection.39
The indication for carotid resection is based on preoperative imaging such as magnetic resonance imaging (MRI) and computed tomography (CT). When studies suggest carotid involvement with no evidence of distant metastases (DM) consideration for carotid artery resection is given and a preoperative assessment is made to determine the patient’s risk for cerebrovascular accident when perfusion is interrupted during this procedure. A balloon occlusion study is often performed preoperatively in order to determine the patient’s ability to temporarily tolerate complete obstruction of blood flow through the carotid artery. If the patient is able to tolerate a balloon occlusion study, then they are considered a candidate for a carotid artery resection. If the patient is not able to tolerate the balloon occlusion study, then the consideration of a carotid artery resection is no longer a viable surgical alternative.
There are only a limited number of publications discussing the outcomes of a carotid artery resection during treatment for head and neck cancer. Brennan et al. reported their 10-year experience of carotid artery resection without revascularization in advanced squamous cell carcinoma of the neck.40 Seven patients underwent elective carotid artery resection, and all seven specimens showed invasion of the carotid artery fascia on pathological exam. Cerebrovascular accident occurred in two patients and the perioperative mortality was 29%.40 The 5 remaining patients all died of locoregional recurrence or metastatic disease within 1 year after surgery.40 The largest series reported in the literature is by Sessa et al. with 30 procedures reported.41 In this series, a 35% DFS rate at 2 years was reported.41 In 2001, Katsuno et al. performed a retrospective review via a computer search of all articles published in the English literature dealing with carotid artery reconstruction for head and neck cancer from 1987 to 1998.42 Studies of patients who underwent a carotid artery resection without a reconstruction were excluded and case reports were excluded. Only 11 articles met criteria for inclusion allowing for a total of 148 patients to be compiled in this series.42 Major neuromorbidity was 4.7% and mortality was 6.8% and the combined major neuromorbidity and mortality were 10.1%.42 The oncologic outcomes were surprisingly interesting. Four of 10 patients from one of the series were reported as disease free for >2 years.43 The Sessa series reported a 35% DFS rate at 2 years.41 Other articles also reported justifiable oncologic results.37,44,45,46
ELECTIVE MANAGEMENT OF THE CLINICALLY NO NECK
The basis and need for elective nodal treatment in head and neck cancer have been based largely on surgical series evaluating pathologic nodal involvement found on elective neck dissection in patients with clinically negative necks. In a consecutive series of 1,081 head and neck cancer patients undergoing radical neck dissection, the incidence of pathologic node involvement was 33 % among those undergoing elective neck surgery.47 The pathologic findings identified the nodal stations at risk by tumor site to establish the rationale for SND as the elective surgical procedure.
Several reports have summarized the risk for metastases and nodal stations at risk.24,48,49,50,51 Some general observations from such data can be made. Regarding larynx cancers, Candela reported the Memorial Sloan Kettering Cancer Center experience in determining the patterns of cervical nodal metastases in 247 larynx cancer patients undergoing 262 radical neck dissections.52 Seventy-eight underwent elective radical neck dissection whereas 118 underwent immediate radical dissection for clinically node-positive disease. The majority of patients (n = 189) were supraglottic larynx and 58 were glottic. Pathologic nodal involvement was found in 37% undergoing elective neck dissection. It is noted that cervical nodes spread in a similar fashion whether the patients are clinically node negative or positive with predominant involvement of level II and III jugular nodes. In clinically node-negative patients, the incidence of involvement of level I and V is <5% with <10% involvement of level IV. In node-positive patients, the incidence of level IV node increases from 15 % to 31% with greater involvement of levels II and III. In clinically node-positive patients, very rarely did patients present with isolated level I nodal metastases without involvement of the jugular nodes.
Similarly, Shah and Candela reported that among oropharynx or hypopharynx cancers treated with elective radical neck dissection occult metastases are found in 26% and that level I and V were involved in only 1.4%, always in association with nodal disease at level II to IV.47,52 No skip metastases were reported. Among oropharynx patients, levels II to IV were predominantly involved, and in the hypopharynx lesions, the primary levels involved were levels II and III. In patients clinically node positive undergoing therapeutic neck dissection, the incidence of level I and V involvement increased to about 10% to 15%; however, levels II to IV were predominantly involved (Table 14.2). Level V involvement only occurred in association with nodal involvement at levels II to IV whereas the incidence isolated level I involvement without levels II to IV involvement (“skip metastasis”) occurred in 0.4%. Thus, based on these studies, elective treatment of the neck in oropharynx or hypopharynx can be directed at levels II to IV.
TABLE 14.2 Percentage Incidence and Distribution of Pathologically Involved Nodes in a Clinical Node-Positive after Therapeutic Radical Neck Dissection
I
II
III
IV
V
Oropharynx n = 165
14
71
42
28
9
Larynx n = 183
7
57
59
29
4
Hypopharynx n = 104
10
76
73
46
11
Oral cavity n = 324
46
43
33
15
3
Source: From Shah JP. Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg. 1990;160(4):405—409, with permission.
Among oral cavity patients, the incidence of nodal disease was 34% on elective evaluation. The majority of metastatic nodes involved levels I to III with only 1.5% incidence of skip metastasis to level IV. Level V involvement is found in only 0.5% with occult disease simultaneously involving other levels. Among those undergoing therapeutic neck dissections, the incidence of level IV involvement increased to 20% while that at level V was 4% always restricted to lower gum or floor of mouth primary sites.
The need for elective treatment not only relates to the estimated probability of nodal involvement and usually is implemented when the risk is 20% or greater but also relates to the morbidity of such treatment as well as the adequacy of coverage. Table 14.3 demonstrates the incidence of nodal involvement of the most common head and neck cancer sites. It should be noted that such data are invaluable but do not address areas that are not addressed surgically, such as the retropharyngeal or pretracheal nodal basins.
Elective nodal treatment by radiation or surgery both offer distinct advantages as radiation may add more comprehensive nodal coverage including the contralateral neck and in regions difficult to surgically address such as the retropharyngeal nodes, inner mandibular nodal areas, and high subdigastric near the exit of the facial nerve at the mastoid process. However, surgery offers important pathologic data, which is useful prognostically, and tailors further therapy according to risk stratification. It should be noted that no randomized or comparative studies of observation versus neck dissection versus ENI have been reported, nor will likely be completed.
TABLE 14.3 Percentage Incidence and Distribution of Pathologically Involved Nodes in a Clinical Node-Negative Neck after Elective Radical Neck Dissection
I
II
III
IV
V
Oropharynx n = 48
2
25
19
8
2
Hypopharynx n = 24
0
13
13
0
0
Larynx n = 79
5
19
20
9
2.5
Oral cavity n = 192
20
17
9
3
0.5
Source: From Shah JP, Candela FC, Poddar AK, et al. The patterns of cervical lymph node metastases from squamous carcinoma of the oral cavity. Cancer. 1990;66(1):109-113, with permission.
Elective Surgical Treatment
Byers reported a series of patients undergoing elective treatment with SND demonstrating excellent outcomes and thus establishing this procedure as a standard of care for elective treatment.53
Retrospective studies point to an improvement in disease-specific survival with the addition of elective neck dissection. Piedbois et al. reported a retrospective comparative study of 233 patients with early stage oral cavity carcinoma with the primary site treated with an interstitial iridium-192 (192Ir) implant who underwent either elective neck dissection or neck observation resulting in two cohorts of patients for analysis.54 This resulted from a change in departmental policies minimizing the impact of potential selection biases. Neck dissection revealed metastases in 25% who then received postoperative radiotherapy. Among those observed, 17% developed a neck relapse with salvage surgery successful in 62 %. Some patients were unable to undergo surgery because of unresectability of disease or poor patient performance status. The 10-year survival was 37% and 31%, respectively, with regression analysis demonstrating that neck observation was associated with an adverse risk for disease-related mortality (p < 0.04). Haddadin et al. reported on a retrospective analysis of 137 patients with T1 to T2 NO oral tongue carcinomas with at least 2 years of follow-up who either received an elective neck dissection, neck observation with salvage therapeutic neck dissection, or no neck surgery at all.55 The cohort receiving elective neck dissection had a superior 5-year cause-specific survival compared with the two other groups despite a negative bias due to a greater proportion of pathologic upstaging of the primary tumor and clinical T2 lesions.
Two randomized studies of patients with early stage oral cavity lesions failed to show a survival benefit in patients randomized to receive elective neck dissection compared to observation with salvage neck dissection if nodal disease developed. In one study, the primary site was managed with primary brachytherapy whereas in the other study the primary site was managed with radical resection.56,57 In the Vandenbrouck study, a 49% incidence of nodal involvement was reported in electively treated patients whereas nodal disease subsequently developed in 47% in the observation group. In the observation arm, the nodal disease appeared to become more aggressive with a higher incidence of extracapsular extension (25% vs. 13%) compared to the electively treated patients and 10% of patients could not undergo therapeutic dissection. However, no survival difference could be detected between the two groups. The authors recommended observation in patients with early stage lesions who could be followed regularly. In the second study of early stage oral tongue cancers, patients undergoing hemiglossectomy and elective neck dissection showed no difference in DFS or overall survival (OS) compared to patients undergoing hemiglossectomy alone.57 The number of patients enrolled on these trials was small and not powered to show equivalence of survival.
Elective Nodal Irradiation
The efficacy of elective nodal irradiation (ENI) is largely based on single institutional studies demonstrating reduced neck relapse.48,58 Fletcher established the dosimetric basis for elective nodal treatment and the need for comprehensive treatment. Delivering elective doses of 50 Gy to a clinically negative neck results in neck control in 95%.58 At a dose of 50 Gy in 5 weeks, the incidence of neck failure was 0% whereas doses of 30 to 40 Gy were associated with regional failure in 9% to 10.5%.58 Further support for ENI is reported by Mendenhall who reported a retrospective review of 125 patients with squamous cell carcinoma of the oral cavity, the oropharynx, the nasopharynx, the hypopharynx, and the supraglottic larynx with a clinically negative neck and control at the primary site.48 The neck failure rate was 1.9% with ENI and 18% without ENI. Among a group of patients expected to have a <20 % risk for occult nodal metastases, the neck relapse rate was 13% in patients who did not receive ENI versus 6% in patients who received ENI. Similarly, among a group of patients with an expected risk for occult nodal metastases >20%, the neck relapse rate was 31% and 5 %, respectively. In a separate report, Mendenhall et al. demonstrated 100% disease control after ENI with 50 Gy in 25 fractions and 99% at a dose of 40.5 Gy in 15 fractions both given as daily fractions.59
Vergeer reported on a large Dutch experience evaluating the benefit of elective radiation therapy treatment of a NO neck. Nodal irradiation was delivered to 785 NO hemi-necks in 619 head and neck patients. Necks were clinical NO (cNO) in 558 and pathologically NO (pNO) in 227. About 47% of patients were oral cavity and well balanced between the two subgroups, with more larynx (22 vs. 13.6) and fewer oropharynx (25 vs. 31%) and hypopharynx (5.7% vs. 7.5%) in the pNO subgroup. Positive margins were noted in 17.0% versus 21.5% along with greater proportion of T3/4 (77% vs. 59%) in the pNO group. Patients were treated with a radiotherapy dose of 46 to 50 Gy. At 3 years, the regional failure for the entire cohort was 5% with a trend toward greater failure in the cNO of 6% versus 3% in the pNO (p = 0.08) and 10% in the ipsilateral neck compared to 4% in the contralateral neck (p = 0.006). Positive margins at the primary site increased the risk of regional failure in the ipsilateral cNO neck to 22% but not in the contralateral cNO neck, where it was 4%, and was significantly higher than those with close or negative margin with regional failure <1%. On multivariate analysis, the laterality (ipsilateral), positive margin status and clinically staged necks had worse regional failure.
Based on older radiation-delivery techniques, traditional ENI involves treatment of bilateral necks with generous coverage of the jugular nodes and major salivary glands with various degrees of coverage of the retropharyngeal, level I and level V nodes depending on the primary site. With the advent of IMRT, such comprehensive coverage can be duplicated or tailored much more extensively. The ability to treat lymphatic areas more discriminately has challenged radiation oncologists to integrate clinical judgment, experience, and understanding of the surgical data to adequately plan regional coverage that it is tailored appropriately for each case. There have been several excellent reviews regarding the delineation of lymph node target volumes indicated for head and neck radiation therapy.14,15,51,60 These summaries have served as a basis for axial-based image treatment planning guidelines that is used for conformal irradiation and IMRT.51 In general, surgical levels defined by Robbins et al. (America Academy of Otolaryngology-Head and Neck Society) are used as the basis for regional target delineation.61 However, there are a wide variety of radiographic landmarks that have been proposed.51,60,62,63 A transatlantic consensus has been reported for the electively treated neck as well as the clinically involved and postoperative neck. Gregoire et al. provide a summary recommendation of the nodal groups that should receive ENI in the neck without altered lymphatic flow (see Fig. 14-1; Table 14.4A).51 These recommendations do not address specific presentations that may modulate the risk for occult metastases. It has been accepted in practice that a risk for <20% warrants at least a deliberation for ENI considering the competing issues of potential benefit and toxicities and risk for secondary HNSCC requiring further therapy.
Elective Surgical versus Radiation Therapy Treatment
The efficacy of ENI versus elective neck dissection showed no obvious differences as reported by Barkley in a major retrospective experience of neck management in 596 patients with oropharynx, larynx, or hypopharynx carcinoma treated at MD Anderson Cancer Center.64 Two hundred thirteen were oropharynx, 202 larynx, and 181 hypopharynx. Of these, 226 were NO whereas 370 were node positive. Patients underwent radiation therapy (n = 292), surgical management (n = 199), or combined modality therapy (n = 105) of the neck. All patients had a minimum follow-up of 2 years and a median follow-up of 4 years. Among the electively treated patients, regional control was >90% regardless of the treatment approach as long as comprehensive neck treatment was implemented. However, partial treatment of the neck resulted in 15%, 35%, and 20% regional failure after radiation, surgery, or combined therapy, respectively.
RECOMMENDATIONS REGARDING ELECTIVE TREATMENT OF COMMON HEAD AND NECK CANCER SITES
Given the significant risk for occult nodal involvement, the standard of care has evolved to electively treat such patients despite the lack of confirmatory randomized trials. Nodal coverage of levels I to III for oral cavity tumors and levels II to IV for oropharyngeal, hypopharyngeal, and laryngeal tumors are mandatory as elective treatment24,47,52,65,66 (Table 14.4B). Elective nodal irradiation including the retropharyngeal lymph nodes is added for primary tumors involving the nasopharynx, tonsil, pharyngeal wall, and the soft palate. Bilateral ENI should be considered for tumors arising from or extending to midline structures such as the soft palate, the base of tongue, and the pharyngeal wall. Tumor sites such as the hypopharynx and the supraglottic larynx require bilateral ENI regardless of the specific tumor stage given high risk for contralateral nodal involvement. In contrast, tumor involvement of ipsilateral structures such as the parotid, the buccal mucosa, and selected tonsil cancers warrants consideration of ipsilateral ENI.67,68 Elective nodal irradiation including level IV lymph nodes should be considered in those with tumors involving the tip of the oral tongue due direct drainage to this area that bypass the orderly contiguous progression in the anterior jugular nodes.47,69 Involvement of the ipsilateral level V lymph nodes in node-negative oral cavity tumors is rare, occurring in <1%, and does not warrant ENI. However, with increasing involvement of levels I to III or the involvement of level IV, the risk for level V involvement increases warranting ENI. In contrast, involvement of only the true vocal cords does not warrant ENI due to the paucity of lymphatic drainage.
IPSILATERAL NECK RADIATION IN LATERALIZED OROPHARYNX CANCER
O’Sullivan et al. reported the results of a large retrospective review which identified oropharyngeal tumors that could be spared by contralateral ENI.67 Two hundred twenty-eight patients with tonsillar carcinomas were treated with ipsilateral radiotherapy at Princess Margaret Hospital. Eligible patients typically had T1 or T2 tumors (191 T1-2, 30 T3, 7 T4) with NO (133 NO, 35 N1, 27 N2-3) disease. Radiation was typically delivered with wedged pair Cobalt beams and ipsilateral low anterior neck field delivering 50 Gy in 4 weeks to the primary volume. At a median follow-up of 5.7 years, the 3-year local control rate was 77%, regional control 80%, and cause-specific survival 76%. Contralateral neck failure occurred in 3% (8/228). All patients with T1 lesions or NO neck status had 100% contralateral neck control. Patients with a 10% or greater risk of contralateral neck failure included those with T3 lesions, lesions involving the medial one-third of the hemi-soft palate, tumors invading the middle third of the ipsilateral base of tongue, and patients with N1 disease. In the presence of ipsilateral node metastases, the risk for contralateral neck failure was 9.5%, 14%, and 21% (all crude rates) for involvement of the soft palate, the base of tongue, and both structures, respectively. However, the authors appropriately note the limitations of these observations as they included patients with uncontrolled primaries and involved a total of only eight patients with contralateral neck failures. Despite this, the report provides confidence in the selection of patients with T1 NO tonsil carcinomas (as well as selected patients with more advanced disease) for only ipsilateral ENI. Similar observations were also reported by Jackson et al. further supporting these observations.70
TABLE 14.4A Consensus Guidelines for Target Delineation of Nodal Levels in the Elective Treated Neck
Level
Cranial
Caudal
Anterior
Posterior
Lateral
Medial
IA
Geniohyoid muscles
Hyoid bone
Symphysis menti
Hyoid bone
Medial edge of anterior belly of digastric
Midline
IB
Mylohyoid muscles cranial edge of SMG
Hyoid bone
Symphysis menti
Posterior border of SMG
Medial border of mandible
Lateral edge of anterior belly of digastric
IIA
Inferior border of lateral process of C1
Inferior edge of hyoid
Posterior bord of SMG
Posterior edge of IJV
Medial edge of SCM
Medial border of ICA
IIB
(As Ha)
Inferior edge of hyoid
Posterior edge of IJV
Posterior border of SCM
Medial edge of SCM
Medial edge of ICA/deep cervical muscles
III
Inferior edge of hyoid
Inferior edge of cricoid
Anterior edge of SCM
Posterior edge of SCM
Medial edge of SCM
Medial ICA/deep cervical muscles
IV
Inferior edge of cricoid
2 cm superior to SCL joint
Anterior edge of SCM
Posterior edge of SCM
Medial edge of SCM
Medial ICA/deep cervical muscles
Va
Superior edge of hyoid
Inferior edge of cricoid
Posterior edge of SCM
Anterior border of trapezius
Platysma
Paraspinal muscles
Vb
Inferior edge cricoid
Transverse cervical vessels
Posterior edge of SCM
Anterior border of trapezius
Platysma
Paraspinal muscles
VI
Inferior border of thyroid
Manubrium
Platysma
Common carotid artery
SCM
trachea
Retropharyngeal
Skull base
Top of hyoid bone
Pharyngeal constrictor muscles
Prevertebral fascia
Medial border of carotid artery
Midline
Retrostyloid
Jugular foramen
Inferior border of lateral process of C1
Paraphageal space
Vertebral body/skull base
Parotid space
Lateral edge of RP nodes
Supraclavicular
Lower border IV/Vb
Sternoclavicular joint
Skin/SCM/clavicle
Anterior edge of postscalenus muscles
Lateral edge of posteriorscalenus muscles
Trachea/thyroid gland
TABLE 14.4B Guidelines for Neck Treatment in Patients with Head and Neck Squamous Cell Carcinomas: Echelons of Lymph Nodes to Be Treated
Primary Tumor Sit
Stage NO-N1
Stage N2-3
Oral cavity
I, II, III, and IV (for anterior tongue tumors only)
I, II, III, IV, and V (may omit if only levels I-III are involved)
Oropharynx
II, III, IV, and retropharyngeal node
I, II, III, IV, V, and retropharyngeal nodes
Hypopharynx
II,a III, IV, and VI (for esophageal extension only)
I, II, III, IV, V, retropharyngeal nodes, and VI (for esophageal extension only)
ELECTIVE NODAL IRRADIATION FOR MAXILLARY SINUS CANCER
Traditionally, ENI has not been routinely considered for maxillary sinus carcinomas due to the low incidence of nodal disease at presentation. However, several investigators have suggested a benefit of ENI for locally advanced NO squamous cell carcinoma of the maxilla.71,72,73,74 Le et al. reported a retrospective review of 97 patients with maxillary sinus carcinoma treated with primary radiotherapy or postoperative radiation at UCSF and Stanford.73 Squamous cell histology was the most common with 60% (58/97), followed by adenoid cystic carcinoma in 20% (19/97) and undifferentiated carcinoma in 16% (16/97). Eighty-nine patients had T3-4 lesions with T2 in eight patients whereas 11% (11/97) presented clinically with nodal disease. Of these 11, one was treated with combined neck dissection and post-op radiation whereas 10 were treated with primary radiation to a median dose of 63 Gy. Of the 86 clinically node-negative patients, 25 patients received ENI (median dose 50 Gy) to the bilateral upper neck nodes. The 5-year actuarial risk for nodal relapse was 0% in patients receiving ENI and 20% for those not receiving ENI. The most common site of nodal relapse was in the ipsilateral level I and II nodal groups with a small number of regional failures in the ipsilateral parotid and upper level V nodes and no instance of failure at level III/IV or supraclavicular nodes. There was no association between primary recurrence and risk for neck failure. However, on multivariate analysis, there was significant association between neck failure and incidence of distant metastasis with higher risk after neck recurrence compared to those regional controlled (82% vs. 19%, p = 0.02). The influence of selection bias with regard to these results is unclear. However, it is likely to have biased against the efficacy of ENI because those patients receiving ENI were likely to have had more advanced disease. Only 1 of 10 patients with neck relapse was salvaged. Of greater significance was the observation that the 5-year actuarial risk for DM was 29% for patients with neck control and 81% for patients with neck failure. Multivariate analysis demonstrated that T stage, N stage, and regional nodal control (HR = 4.5, p = 0.006) independently influenced this risk. The 5-year survival was 37% and 0% for patients with neck control and neck relapse, respectively (p = 0.3). Late complications arising from neck irradiation occurred in 1 of 36 patients who developed ipsilateral brachial plexopathy and severe neck fibrosis. In light of the relapse pattern, the investigators concluded that ipsilateral ENI to only the upper neck (levels I and II) be considered for patients with T3 and T4 NO squamous cell carcinoma of the maxillary sinus. Similar conclusions were reached by other investigators.23,25
MANAGEMENT OF THE CLINICALLY NODE-POSITIVE NECK (N+)
Management of the clinical positive neck is controversial with a wide variety of approaches that mirrors the complexity and competing regimens established to treat the primary site. These include neck dissection followed by postoperative radiation; definitive concurrent chemoradiation, radiation, or concurrent chemoradiation followed by planned or salvage neck dissection; and induction chemotherapy followed by neck dissection before or after radiation. Refinements in the radicality of neck dissection (radical vs. modified vs. selective vs. super selective neck dissection) and the identification of patients at high risk for recurrence, development of consensus guidelines in nodal target delineation for intensity-modulated treated patients, radiation dosing, and fractionation as well as integration of chemotherapy have been issues that have been explored to maximize regional control and preserve quality of life and function. The manner in which the primary site is managed guides treatment of the neck. Thus, relevant considerations in the decision include the resectability of the primary and neck disease, the functional morbidity incurred by surgery or radiation at the primary site, and the appropriateness of the primary lesion for potential organpreserving therapy with either radiation alone or in combination with chemotherapy. When unresectable disease exists, the use of chemoradiation strategies has largely been favored. Although the optimal chemoradiotherapy regimen for both organ preservation and unresectable disease remains to be defined, the bulk of the data favor concurrent chemoradiation whereas more recent data point to possible additional benefit of induction chemotherapy or to integration of biologic therapies. Following these therapeutic considerations for the primary lesion, the principal issue with regard to neck management has been the necessity of adjuvant postoperative radiotherapy/chemoradiation or postradiotherapy/chemoradiation neck dissection.
Surgery and Postoperative Radiation
Surgery and postoperative radiation remains a common strategy for regional management especially for the majority of resectable oral cavity tumors and many locally advanced but resectable HNSCC such as bulky or cartilage invasive hypopharynx or larynx cancers. More recently with early and intermediate stage oropharynx cancer, transoral robotic surgery is used increasingly followed by neck dissection. Historically, radical neck dissection alone had been the mainstay of regional treatment with radical extirpation of the neck nodes and adjacent nonlymphatic structures with significant functional and cosmetic morbidity as described by Crile in 190375,76 and reintroduced in the 1950s by Martin.77 However, it was well recognized that recurrence in the neck after radical neck dissection carried an ominous prognosis.78 Large series evaluating risk factors for recurrence after neck dissection have been reported. Of these, the most consistently reported risk factor for recurrence is extracapsular extension (ECE). Snow et al. reported one of the first important large institutional experience using pathologic factors to predict risk of recurrence. In a series of 405 patients, he reported that the presence of extracapsular extension of nodal disease was the single most important predictive factor on multivariate analysis for neck recurrence and poor survival.79 Furthermore, he noted that although there was a relationship between node diameter and fixation with ECE as >75% of nodes >3 cm and 70% with fixation had ECE, these parameters themselves were not sufficient as 20% of nodes <1 cm had ECE and 30% with nodal fixation had no ECE.79 Carter et al. reported an extensive analysis of 250 radical neck specimens and their clinical significance.80 Both the presence and the extent of ECE was found to be the most important factor predicting for neck relapse with a distinction between macroscopic and microscopic ECE emphasized with the former having a worse prognosis.80 Others have verified such findings.80,81,82 and reported other poor prognostic pathologic factors including lymphvascular invasion,1 perineural invasion,83 number of nodes involved,79,84 as well as nodal level involved.64,84,85,86,87,88 Risk factors for recurrence based on findings from primary site include most importantly the status of the resection margins89,90,91,92 as well as the primary tumor site origin.93,94
Postoperative head and neck radiation therapy was pioneered by Fletcher, who laid down the principles of treatment fields and time-dose factors.95 He demonstrated that 50 Gy offered excellent control rates as elective treatment but greater doses were needed to control high-risk disease in a postoperative setting.90 Moreover, he reported the importance of comprehensive treatment of the entire neck and primary site either as adjuvant or as salvage for gross residual disease given that localized radiation was associated with high rates of locoregional failure including contralateral neck compared to comprehensive radiation of the primary and whole neck (locoregional failure 73% vs. 58%, respectively).95 Thus, the majority of studies in the postoperative setting have evaluated the benefit of radiation as a locoregional treatment for indications based on high-risk features from either the primary site or neck.
Postoperative radiation (PORT) appears to benefit patients with extracapsular extension compared to resection alone. In a retrospective review of 405 patients treated at the Netherlands Cancer Institute, Bartelink et al. reported that PORT decreased recurrence and improved survival compared to surgery alone in the cohort of patients with ECE but no preoperative fixation of lymph nodes.96 Similarly, Huang et al. reported superior survival rates in a retrospective review of a more homogeneous cohort of 125 patients with high-risk features (ECE or positive resection margin) treated with either surgery and PORT or surgery alone.48 Factors demonstrated to independently influence survival included the use of PORT (p = 0.0001) and the number of lymph nodes with ECE (p = 0.0001).97 Despite the use of PORT, the number of lymph nodes with ECE remained significant attesting to the adverse influence of this pathologic feature. This study is significant because the two study populations resulted from the management bias of the operating surgeons to prefer or not to prefer PORT. This clearly defined treatment choice limits the selection bias that often confounds retrospective analyses. Others have reported the locoregional benefit of PORT in patients with multiple positive nodes.98,99,100
Postoperative radiation has consistently been shown to decrease locoregional failure53,64,85,87,101 but its impact on survival is less conclusive as some retrospective studies report a survival benefit whereas others report only an alteration in failure pattern toward distant metastasis but no survival benefit.85,102,103 Mishra et al. reported on the randomization of 140 patients with stages III and IV (T3-T4, N0-N2B) buccal mucosa carcinoma to PORT (mean dose 60 Gy) or observation following surgical resection.104 A significant improvement in the DFS was observed in favor of PORT (68% vs. 8%, p < 0.005) after a minimum follow-up of 36 months. This observation is noteworthy given the selection bias against the PORT arm that resulted from a biased randomization process due to surgeon preference, yielding a greater proportion of advanced node-positive disease in the PORT arm. Kokal et al. reported the preliminary results of a potentially underpowered randomized trial of 51 patients with stage III and IV squamous cell carcinoma arising from the oral cavity, the larynx, and the pharynx treated with surgery or surgery and adjuvant PORT (50 Gy).105 The study excluded randomizing patients in the postoperative setting if the resection margins were positive or there was clinical evidence of nodal metastases, hence largely evaluating the role of PORT for pathologic nodal metastases. A median follow-up of 30 months was reported. No differences in locoregional control in the primary site and ipsilateral neck was observed (22% vs. 26%) in the surgery alone versus postoperative radiation group. However, fewer contralateral undissected neck recurrences (5.3% vs. 14.8%, crude rates) and fewer DM (5.3% vs. 14.8%, crude rates) were observed in favor of the cohort receiving PORT. This resulted in a nonsignificant difference in the actuarial relapse rate and 3-year OS rate (37% vs. 68%, p = 0.16 and 58.5% vs. 46.5%, p = 0.31, respectively) in favor of the irradiated group.
A matched pair analysis of patients treated at the Mayo clinic demonstrated a benefit of postoperative radiation in dissected patients.106 Matched pair analysis was drawn from two pools of patients. One consisted of 95 consecutively treated patients undergoing neck dissection and postoperative radiation therapy (bilateral neck irradiation; median dose 56 Gy) treated from 1974 to 1990. The other cohort consisted of 284 patients treated by neck dissection only between 1970 and 1980. Patients were matched by nodal stage, age, gender, number of nodes involved >4, desmoplastic nodal pattern, which had been highly predictive for neck recurrence at this institution. A total of 56 matched pairs were compared. The relative risk (RR) for recurrence on the unilaterally dissected side, any neck recurrence, cancer-related death and death from any cause were 5.82, 4.72, 2.21, and 1.67 in the surgery alone arm compared to those receiving postoperative radiation. Although extracapsular extension was not specifically studied, the authors reported a high correlation between desmoplastic nodal pattern and ECE, suggesting the growth pattern may be a reasonable surrogate for ECE. With regard to absolute outcomes in the 95 patients receiving radiation therapy, the regional failure was 26 % at a median follow-up of 4.5 years whereas the 5-year disease-specific survival and OS were 64% and 39%, respectively, consistent with other postoperative experiences. Frank et al. also reported an improvement in both OS and DFS in a retrospective comparative review of 110 patients with carcinoma of the hypopharynx treated with either surgery alone or followed by PORT.107 Despite the presence of more advanced disease, the cohort receiving PORT was demonstrated to have a superior locoregional relapse rate (14% vs. 57%, p < 0.0001), DFS, and adjusted 5-year survival (48% vs. 18%, p = 0.029). Treatment with PORT was an independent prognostic factor in multivariate analysis for both DFS (p = 0.0009) and OS (p = 0.0289).
Several retrospective studies have reported the effectiveness of achieving neck control by nodal stage, and selected reports from large U.S. centers are illustrated in Table 14.5.64 Conventional postoperative radiation offers excellent control in N1 patients, acceptable results in the N2 neck and suboptimal outcomes after N3 treatment. Vikram reported improved regional control after postoperative radiation in patients with one or multiple nodal stations involved and emphasized the importance of minimizing treatment delay.101 A series of 114 patients treated with surgery and postoperative radiation were compared to historic control treated with similar surgical techniques (radical neck dissection). Seventeen percent were found to have nodal metastasis at one level whereas 66% had disease at multiple nodal levels. Patients were treated with postoperative doses of 50 to 60 Gy over 5 to 6 weeks. The crude regional failure rate among patients with positive nodal disease treated with postoperative radiation was 10%. Compared to patients treated with surgery alone, the regional failure rate after postoperative radiation was decreased whether disease was localized at a single nodal level (regional failure 16% vs. 36.5%) or if multiple levels of nodes were positive (13% vs. 72%) and also appeared better than another cohort treated with preoperative radiation to a dose of 20 Gy (regional failure 28% [single nodal level] and 37% [multiple nodal levels]). Regional failure was greater in patients starting radiation 6 weeks postoperatively compared to those starting radiation within 6 weeks (2% vs. 15%, p < 0.02). This time interval of >6 weeks negatively impacted on regional control whether single-level nodal involvement (regional failure 33% vs. 0%) or multiple levels of nodes were involved (27% vs. 3%). Others have also demonstrated the importance of minimizing the total treatment package time.108,109,110
TABLE 14.5 Single-Institution Series of Radical Neck Dissection and Postoperative Radiation-Neck Control by N Stage
MDAC, Mental Disability Advocacy Centre; OPX, oropharynx; LX, larynx; HPX, hypopharynx; OC, oral cavity; UFLA, University of Florida; MSKCC, Memorial Sloan-Kettering Cancer Center.
Unilateral Postoperative Radiation Therapy in Oral Cavity Cancer
Vergeer reported the experience of treating 123 oral cavity cancer patients with lateralized tumors who underwent resection and unilateral postoperative radiation. A lateralized tumor was defined as >1 cm from midline. Patients were treated to the primary tumor bed in all cases, which included the ipsilateral neck in 90%. Tumors involved the oral cavity primarily including the gingival, the oral tongue, the floor of mouth, the buccal mucosa, and the floor of mouth in 104 patients with T1-4 and node-positive disease in 62%. The median total doses to the primary site involved nodal station, and elective nodal areas were 63 Gy, 66 Gy, and 46 to 50 Gy, electively. At a minimum follow-up of 5 years, a total of seven patients failed contralaterally with a 5-year actuarial failure rate of 8%. The risk of contralateral nodal failure rate was related to the pretreatment nodal stage (p = 0.008) and occurred in 1%, 12%, and 27% in patients with pNO, pNl-N2a, and pN2b, respectively. Of the seven contralateral nodal failures, five were salvaged with neck dissection. The presence of extracapsular extension was of borderline significance (p = 0.06) for increased risk of contralateral nodal failure (14% vs. 6%, p = 0.081). The benefit of unilateral radiation therapy was the low rate of morbidity. At 5 years, the incidence of cumulative RTOG chronic grade 2 to 4 xerostomia was 20%, grade 3 mucosal complications 9%, grade 3 to 4 bone complication 17%, and grade 3 to 4 fibrosis 23%.
Special Issues Regarding a Solitary Node
In patients with a single histologically positive node without extracapsular spread, the regional recurrence rate may not warrant radiation therapy. In the study by Carter et al., where ECE is present in a solitary lymph node, the 3-year neck relapse rate was found to be 25%.80 Where ECE is absent, Barkley et al. noted neck relapse in 5 of 47 (11%) patients with N1 disease treated with surgery alone compared with a comparable retrospective cohort of 21 patients that received PORT with no neck relapse observed.64 Hence, neck irradiation is commonly recommended in the setting of ECE, reserving neck observation where no ECE is present and the patient is likely to remain compliant to a course of close observation. After SND without radiation, the regional recurrence rates ranges from 4% to 10% and did not appeared to be improved with the addition of radiation. However, others note the poor outcomes after recurrence in a dissected neck and favor treatment.53,98,111,112,113,114
For patients having undergone a local excision of a solitary node, the adequacy of radiotherapy in the management of a neck with potentially a higher burden of residual microscopic disease has been reported.115,116 Mack et al. reported on 41 patients referred for irradiation following excision of a solitary neck metastasis with no gross residual disease.116 The N stage was Nx (n = 7 patients), N1 (n = 15 patients), N2A (n = 18 patients), and N3A (n = 1 patient). Neck irradiation was administered with doses ranging from 5,485 cGy to 8,100 cGy (median dose, 6,675 cGy). A planned neck dissection was administered in two patients. Actuarial neck control was 95% at both 5 and 10 years. Distant metastasis was observed in 0 of 36 patients with disease controlled above the clavicles versus 3 of 5 patients with relapse above the clavicles. Hence, this report would support the efficacy of postexcision radiotherapy to the neck for most patients presenting with solitary N1 or N2A disease without an increased risk for distant metastasis. The efficacy of postexcision radiotherapy for N3A disease is unclear given the higher risk for residual microscopic disease in the neck. A neck dissection would appear to be warranted. Ellis et al. confirm that the potential adverse effects of violating the neck with an open neck biopsy, on both the probability of neck control and the risk for distant metastasis, could not be demonstrated in a regression analysis when radiotherapy was subsequently delivered to the neck.117 In a separate report from the same institution, Parsons et al. also reported on the neck control rates following an open neck node biopsy resulting in patients with or without gross residual disease.115 Gross residual neck disease remained in 55 patients. A neck control rate of 64% was observed when the neck treatment was predominantly with radiotherapy alone. The subsequent consistent addition of a planned neck dissection improved the neck control rates. For N1 to N2 disease, the neck control rate was 65% with irradiation alone and for N2 disease 86% with the addition of a neck dissection. For N3A disease, the neck control rate increased from 29% (2/7) to 63% (5/8) supporting the need for a neck dissection where the burden of residual microscopic disease is increased.
HPV and Need for Completion Neck Dissection in a Violated Neck
Loyo reported on 94 patients treated at Johns Hopkins University or University of Pittsburgh who had an open cervical biopsy and managed with either completion neck dissection (n = 53) or chemoradiation (n = 41). Oropharynx comprised 84% of patients (79/94) and were HPV positive in 87% (55/63). Patients treated with neck dissection had a lower proportion of HPV negative patients (3.7% vs. 14.6%, p = 0.009) compared to those managed nonoperatively. Regional failure rate was similar 2/53 versus 2/41 in patients managed surgically or with radiation, respectively. There appeared to be no difference in 5-year disease-specific survival (82% vs. 85%, p = 0.58) or DFS (82% vs. 70%) in those managed with completion neck dissection versus nonoperative management.
Pre- versus Postoperative Radiation Therapy
The sequencing of radiation therapy either before or after definitive resection was explored in the Radiation Therapy Oncology Group (RTOG) trial 73-03 involving 320 patients of primarily stage III/IV patients.93 Patients with larynx or hypopharynx cancer undergoing radical surgery (n = 211) were randomized to receive 50 Gy preoperatively or 60 Gy postoperatively whereas patients with oral cavity/oropharynx were randomized to three arms: pre- or postoperative radiation or a third arm of definitive radiation therapy (65-70 Gy) only. Results were reported at a median follow-up of 5 years. Of the 277 patients treated with radical resection, postoperative radiation was superior to preoperative radiation in increasing locoregional control (65% vs. 48%, p = 0.04) and trended toward improved OS (38% vs. 33%, p = 0.10). Among the 43 oral cavity/oropharynx treated with definitive radiation therapy, locoregional control was lower compared to those undergoing resection and pre-op or post-op radiation (38% vs. 43% vs. 52%, respectively) but not significantly different likely due to small numbers of patients. Survival was similar (33% vs. 30% vs. 36%, respectively). The rates of severe surgical or radiation complications requiring hospitalization occurred in 15% to 20% and was not significantly different. Thus, this trial appeared confirmed that postoperative radiation is the best treatment sequence for patients undergoing radical resection of the primary site.
Dose Escalation in Postoperative Radiation
Retrospective studies have demonstrated the importance of dose escalation to overcome the greater risk for recurrence for close or positive margins.89,90,92 The value of dose escalation with postoperative radiation was explored in a prospective, randomized trial reported by Peters stratifying 302 radically resected patients as low, intermediate, or high risk for locoregional recurrence based on an empirically derived scoring system evaluating margin status, stage, and pathologic factors.118 Patients were randomized to four dose levels at 52.2 Gy, 57.6 Gy, 63 Gy, and 68.4 Gy to the resection bed whereas 54 Gy was delivered to nonsurgically treated areas of potential subclinical disease. Analysis of 240 patients at a median follow-up of 45 months failed to validate the scoring system but did show that ECE was the overriding risk factor for locoregional recurrence (30% vs. 19%, p = 0.04). For the 110 patients with ECE, a dose of 63 Gy was superior compared to <57.6 Gy (locoregional recurrence 26% vs. 48%, respectively) but there was no further benefit at 68.4 Gy (locoregional recurrence 28%) and more complications. There did not appear to be a comparable increased risk for neck relapses (neck control: <54 Gy, 89%; 57.6 Gy, 86%; 63 Gy, 89%). For patients stratified to the high-risk group, there did not appear to be any significant benefit with regard to neck control rates (84% vs. 77%) when the 63 Gy dose level was compared with the 68.4 Gy dose level. Although these observations may reflect an underpowered analysis, it has been concluded that a dose of at least 63 Gy is warranted to postoperative sites at greatest risk. The study did show that the presence of two or more risk factors predicted a high risk for failure. These factors included the presence of a primary oral cavity site, close or positive surgical resection margins, perineural invasion, two or more metastatic lymph nodes, node diameter >3 cm, a treatment delay to PORT >6 weeks, and a Zubrod performance status of >2. Based on this trial, minimum doses of 57.6 Gy are recommended to the whole operative bed with boost to 63 Gy to areas at high risk, especially where ECE is present.
Altered Fractionated Postoperative Radiation
The value of accelerated postoperative radiation to decrease the total treatment package time was demonstrated in a follow-up multi-institutional randomized trial reported by Ang et al.110 Patients were stratified by risk according to the risk factors identified in the aforementioned study. Patients with no adverse pathologic factors were deemed low risk and not given PORT. Patients with one pathologic risk factor were deemed intermediate risk and treated with conventional fractionated radiation to a dose of 57.6 Gy in 6.5 weeks. Those with ECE or the presence of >2 risk factors were deemed high risk and treated with high-dose conventional radiation to 63 Gy/7 weeks or to accelerated radiation by delayed concomitant boost to 63 Gy/5 weeks. At a median follow-up of 59 months, locoregional control was excellent for low-risk patient who were observed and intermediaterisk patients (5-year actuarial LRC 90% vs. 94%, respectively). High-risk patients had a 5-year actuarial LRC and survival rate of 68% and 42%, respectively. Within this cohort, patients undergoing accelerated postoperative radiation had a nonsignificant improvement in LRC (p = 0.11) and survival (p = 0.08). The value of accelerated treatment was based on the ability to keep the treatment package time to 11 weeks or less as patients who were started with a 7-week conventional course of radiation within 4 weeks of surgery did as well as the accelerated radiation group. These results confirmed that in the absence of adverse pathologic factors, as studied, low-risk patients do not require PORT. In contrast, high-risk patients need a shortened treatment package time.
Post-op Chemoradiation for High-Risk Disease
Sequential Post-op Chemoradiation. The role of chemotherapy has been integrated into locoregional management due to the poor survival outcomes (30%-40%), potential for improved locoregional control from 70% to 80% and distant metastasis in 20% after standard therapies. The concept of synergistic effect of cisplatin-based chemotherapy and radiation has been reviewed.119
The NCI-sponsored Head and Neck Contracts Program multi-institutional phase III trial was conducted between 1978 and 1982 in 462 patients with resectable stage III/IV cancers of oral cavity/larynx/hypopharynx testing the possible benefit of either induction or adjuvant chemotherapy in patients receiving conventional postoperative radiation.120 Patients were randomized to three arms: (a) standard resection and postoperative radiation, (b) induction cisplatin/bleomycin for one cycle followed by standard therapy, or (c) therapy as outlined in (b) followed by maintenance cisplatin chemotherapy for 6 months. Radical neck dissection was performed in node-positive patients. Radiation therapy was delivered with conventional technique to final doses of 60 to 70 Gy for any residual disease. There was no differences in postoperative surgical complications or delays in initiating radiation therapy in chemotherapy patients compared to standard therapy patients. No differences in acute or late radiation toxicities could be detected with the addition of chemotherapy. At a median follow-up of 61 months, the incidence of DM was significantly decreased in patients receiving maintenance chemotherapy (9% vs. 19% vs. 19%, p = 0.025 and 0.021, respectively) compared to the standard and induction chemotherapy patients. The difference in distant metastasis was even more remarkable given that 45% randomized to the maintenance arm did not receive any chemotherapy due primarily to patient refusal, cancer recurrence, or death whereas only 9% received all six cycles. No difference in locoregional control was noted. Overall or DFS in maintenance chemotherapy patients was not statistically significantly increased compared to standard and induction arms (OS: 45% vs. 35% vs. 37%, respectively) and (DFS: 64% vs. 55% vs. 49%, respectively). However, adjuvant chemotherapy is not routinely recommended given the poor compliance and lack of evidence of survival benefit in large meta-analysis.2,3,4,5,121
Intergroup-0034 randomized 442 patients to standard surgery and radiation therapy versus surgery followed by CDDP/5FU chemotherapy for three cycles then postoperative radiation.121 Only patients with negative margins were entered and then stratified according to low or high risk. High-risk patients included those with close surgical margins (<5 mm), extracapsular extension or in situ disease at the margins. For all patients, there was no difference in locoregional control, disease-free survival, or OS. The incidence of first failure in the neck (10% vs. 5%, p = 0.03) and DM (23 % vs. 15 %, p = 0.03) was lower in the chemotherapy arm. However, among patients with high-risk disease, there was a suggestion that chemotherapy did decrease locoregional failure (28% vs. 34%, p = 0.07) and improve OS (50% vs. 39%, p = 0.06).121
Concurrent Post-op Chemoradiation. Based on the Intergroup-0034 study, a high-risk group was identified that might benefit from chemotherapy. The concept of combining chemotherapy concurrent with radiation to provide synergistic benefit and spatial cooperation (radiation to cover locoregional disease and chemotherapy to address systemic micrometastasis) had been proposed and tested in multiple trials using single or polychemotherapy regimens in the definitive setting. Subsequent large meta-analyses demonstrated that the benefit of chemotherapy on survival and locoregional control was largely derived when combined concurrently. Although multiple chemotherapy regimens had been studied, the most consistent to offer a benefit was single-agent cisplatin.
Two landmark studies were organized independently in Europe (EORTC 22931) and in the United States (RTOG 95-01).122,123 Both tested whether the addition of three cycles of high-dose cisplatin concurrent with conventionally fractionated postoperative radiation could benefit patients at high-risk for recurrence. The dose of cisplatin was 100 mg/m2 every 3 weeks while the dose of radiation in the RTOG study was 60 to 66 Gy and 66 Gy in the European Organization for Research and Treatment of Cancer (EORTC) trial. Definition of high risk included extracapsular extension and positive margins in both studies; however, each study had other nonoverlapping eligibility criteria including multiple nodes in RTOG 95-01 and lymphvascular invasion, perineural invasion, stage III/IV disease, or level IV or V nodal involvement in oral cavity/oropharynx primaries in EORTC 22931. The primary endpoint in the RTOG trial was locoregional control whereas progression-free survival was the primary objective in the EORTC study. Table 14.6 compares the patient characteristics and outcomes of both trials. Oropharynx cancers comprised a greater proportion of patients (42% vs. 30%) in the RTOG study whereas the EORTC study had more hypopharynx cancer (20% vs. 10%). More N2/3 patients were entered in the RTOG study (94% vs. 57%). The incidence of ECE was similar between the two studies (RTOG: 53% vs. EORTC: 57%), but more positive margins were noted in the EORTC study (29% vs. 10%). Also, the majority of patients in the EORTC study received 66 Gy whereas only about a tenth of patients in the RTOG study did so. At a median follow-up of 60 months in the EORTC study and 46 months in the RTOG, the addition of chemotherapy improved the primary endpoints. Both studies showed about a 9% to 13 % improvement in locoregional and DFS, with no difference in incidence of distant metastasis. OS was statistically improved in the EORTC study with a 13% absolute improvement at 5 years and trended toward significance in the RTOG trial with a 9% absolute 4-year increase.
TABLE 14.6 Comparison of Phase III Postoperative Chemoradiation versus Radiation