© International Society of Gynecological Endocrinology 2015
Bart C. J. M. Fauser and Andrea R. Genazzani (eds.)Frontiers in Gynecological EndocrinologyISGE Series10.1007/978-3-319-09662-9_2020. Fertility Preservation and Pregnancy After Breast Cancer: When and How?
Nicoletta Biglia1 , Marta D’Alonzo1, Silvia Pecchio1, Maria Chiara Ottino1, Alberto Daniele1 and Guido Menato1
(1)
Department of Gynecology and Obstetrics, University of Torino, Mauriziano Hospital, Largo Turati, 62, Turin, 10128, Italy
20.1 Paper
Breast cancer is the most common malignant tumor in women. Survival has been steadily increasing in the last 15 years, with an actual 5-year survival of 87 %. Around 6 % of breast cancer cases occur in women younger than 40 years. These patients face specific issues compared to older women, including an increased risk of recurrence, inferior survival, and the need of a broader psychosocial support. Issues related to the effects of local and systemic treatments such as the alteration of body image, sexuality complaints, and fertility impairment have a higher priority in this young women population. A recently published EUSOMA recommendation states that fertility issues must be discussed before the start of any type of anticancer treatment and that the optimal type of fertility preservation, endocrine treatment duration, and the effect of subsequent pregnancies on breast cancer prognosis remain research priorities [1].
Currently fertility preservation techniques rely on cryopreservation of embryos, of mature oocytes, and of ovarian tissue and on the administration of GnRHa concomitant to chemotherapy [2]. The first three techniques are a part of a medically assisted reproduction program and require the patient’s referral to a specialized center. Each of these techniques has advantages and disadvantages that must be evaluated considering each single case, but all of them must be carried on before starting oncologic treatments. Embryo cryopreservation is a well-established technique, but the need of a male partner or sperm donor for embryo cryopreservation is a requirement that cannot always be fulfilled. The ethical implications of the increasing number of embryos stored in IVF clinics and law restrictions make other techniques the preferred option for fertility preservation [3]. Oocyte cryopreservation requires ovarian stimulation, mature oocyte retrieval, and subsequent slow freezing or vitrification. Thawing and subsequent intracytoplasmic sperm injection (ICSI) with embryo transfer can be performed years after the procedure. Controversial issues include the delay that this procedure might determine in the beginning of adjuvant therapy and the high estrogen levels reached during the stimulation. The delay is not such a relevant issue considering that ovarian stimulation requires approximately 2 weeks from the beginning of menstrual cycle and several studies of adjuvant chemotherapy suggest no detrimental effects, on survival or recurrence, if chemotherapy is started within 12 weeks after surgery [4]. Concerning the use of gonadotropins in ER+ and in ER− patients, the levels of serum estradiol (E2) during ovarian stimulation could be 30 times higher than those detected in a natural menstrual cycle. The potential detrimental effect of this estrogenic peak generated a vigorous debate on the risk of recurrence not only in ER+ but also in ER− patients. Some authors believe that there is no real risk in having a short-term increase in hormonal levels [5], if this is followed by chemotherapy. Recently, ovarian stimulation protocols with aromatase inhibitors have been proposed in order to avoid high estradiol levels and the recurrence rate of breast cancer does not seem to be increased [6, 7]. Due to the relatively short-term follow-up and the small number of patients, a final statement on the safety of this approach cannot yet be rendered. Azim et al. suggest that the use of letrozole and gonadotropins for controlled ovarian stimulation was unlikely to result in a significant increase in recurrence of breast cancer. Further research, including longer-term follow-up are needed to confirm these findings; in the meantime, the use of letrozole-FSH protocol in women with breast cancer who wish to preserve their fertility by oocyte or embryo cryopreservation is certainly a viable option [8]. Ovarian tissue cryopreservation is still considered an experimental technique but in recent years is achieving interesting results. The pickup of ovarian tissue can be done at any time of menstrual cycle, without delay in starting therapies, and it may be performed laparoscopically. At the appropriate time, when the patient decides to search pregnancy, the orthotropic transplantation has the greatest chances of success [9]. This technique does not require hormonal stimulation and allows the storage of a very large number of follicles. To date, approximately 20 children have been born worldwide after ovarian tissue cryopreservation [3], and the first live birth in Italy took place in February 2012. Some studies showed the effectiveness of associating GnRHa to chemotherapy in preserving ovarian function, probably for the temporary ovarian suppression during the treatment [10], but an international consensus on the gonadoprotective role of GnRHa has not been reached, and ovarian suppression with GnRHa during chemotherapy as a method to preserve fertility remains a highly controversial topic. The very recently updated clinical practice guidelines for fertility preservation in cancer patients released by ASCO in 2013 conclude that, given the current status of knowledge on this issue, GnRHa is not an effective method of fertility preservation, and encourage to include the patients in clinical studies [11]. To the same conclusions, get the ESMO recommendations on cancer, pregnancy, and fertility [12]. The large differences among studies in the definition of amenorrhea and the lack of more standardized and reliable markers of residual ovarian reserve contribute to maintain this debate open. In the largest published randomized study (PROMISE) which included about 300 patients, about 9 % of patients in the GnRHa arm did not resume menses or showed FSH levels in the postmenopausal range after 1 year versus 26 % in the arm with chemotherapy alone [13]. On the other hand, the ZORO study failed to show any protective effect of the concurrent administration of goserelin on the rate of amenorrhea at 6 months, albeit the sample included was much smaller [14].
Concerning the safety and feasibility of pregnancy after breast cancer, many literature data have shown that pregnancy does not affect the prognosis, both in ER+ and ER− patients, even supposing a protective effect of pregnancy. In 2010, a large meta-analysis was published by Azim et al., with data from 14 studies for a total number of 1,244 cases and 18,145 controls. Authors showed a better overall survival (OS) for women who got pregnant following breast cancer diagnosis compared to those who did not get pregnant [HR: 0.59; 95 % CI 0.50–0.70]. Authors hypothesized that these results could present a selection bias, earlier described as the “healthy mother effect” phenomenon, but also the sensitivity analysis, performed including only those studies that had breast cancer controls known to be free of relapse, showed a trend toward improved survival for women who got pregnant, although not statistically significant [HR: 0.85; 95 % CI 0.53–1.35] [15]. Similar results were described by Kranick et al. in the same period, confirming no difference in prognosis, in terms of OS and disease-free survival (DFS) between cases and controls, respectively, for breast cancer patients who get pregnant or not [16]. Recently, these evidences have been confirmed by Azim et al. in another large multicenter study, evaluating the prognostic impact of pregnancy in the subgroup of women with a previous ER+ breast cancer. A total of 1,207 patients were included in the study, 333 women who became pregnant after breast cancer and 874 controls who did not became pregnant. No difference in overall event rate was observed between cases and controls [HR: 0.84; 95 % CI 0.66–1.06; p = 0.14]. Of note, no difference was observed for either ER+ or ER− cohorts. Better overall survival was reported in the group of pregnant patients (p = 0.03), independently from ER status (p = 0.11). Moreover, in this study, breastfeeding and time to pregnancy seemed to have no effect on risk of relapse in women who achieved a term pregnancy [17]. The timing of pregnancy following breast cancer diagnosis is a crucial point. Biological evidence suggests that pregnancy might serve as a fertile soil for incipient lesions in the breast in the short term [18]. A recent population-based study [19] has shown that the risk of death decreases significantly with increasing interval between diagnosis and subsequent childbirth. In an interesting review, Azim Jr. and colleagues [20] found that pregnancy 2 years following breast cancer diagnosis conferred a significant reduction in overall mortality (pooled relative risk: 0.55; 95 % CI: 0.36–0.84; p-value for heterogeneity = 0.16). Therefore, it is common practice that a minimum period of 2 years following diagnosis should be allowed before attempting to get pregnant. For patients with a history of ER-positive breast cancer, 5 years of adjuvant hormonal therapy remains the current standard of care [21], and pregnancy should be postponed to allow the complete endocrine treatment. This allows a reduction in the relative breast cancer recurrence risk and the relative risk of death. A conflict will always remain for those women with ER-positive disease who wants to prematurely stop their hormonal therapy to become pregnant. The best option is to wait until the end of the treatment, with a tamoxifen-free interval of at least 3 months. Nonadherence to tamoxifen therapy, in particular early discontinuation of treatment, is likely to result in worse outcomes, notably in high-risk patients. Comparison of treatment durations indicates that women receiving less than 5 years therapy have higher breast cancer recurrence rates and mortality. Discontinuing tamoxifen after 2–3 years reduces the clinical benefit but allows to satisfy the desire for motherhood in young women; moreover, tamoxifen treatment could be completed after childbirth. If in case of spontaneous pregnancy during tamoxifen use, it should be stopped as soon as possible to avoid its possible teratogenic effects. Finally, before a planned pregnancy is initiated, a complete checkup including clinical breast examination, mammography, ultrasound scan, and, if necessary, MRI should be performed, as well as a complete metastatic workup.
Related posts:
 Management of Adolescent Hyperandrogenism
Management of Adolescent Hyperandrogenism
 Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Supplementation with DHEA in Poor Responder Patients
Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Supplementation with DHEA in Poor Responder Patients
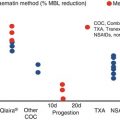 Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
 Low Malignant Potential Tumors
Low Malignant Potential Tumors
 Disorders of the Menstrual Cycle During Adolescence
Disorders of the Menstrual Cycle During Adolescence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


