EFFECTS OF HORMONES ON BONE CELLS
Part of “CHAPTER 50 – PHYSIOLOGY OF BONE“
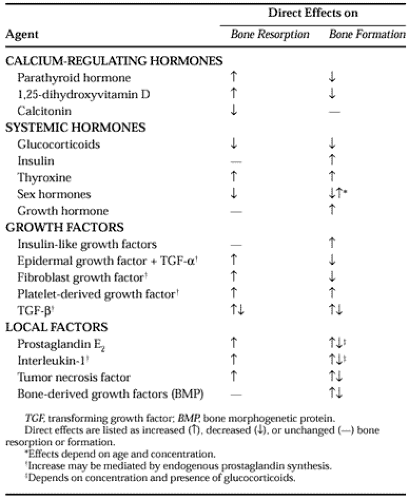
Despite many studies of the direct effects of hormones on bone, the complex regulation of bone resorption and formation still is inadequately explained. The effects of systemic agents are probably modulated by interactions with local intercellular mediators. For example, PTH is clearly a potent stimulator of bone resorption both in vivo and in vitro but has not been shown to act on isolated osteoclasts in the absence of other bone cells. Prostaglandins are also potent stimulators of bone resorption, but they decrease motility and resorptive activity of isolated osteoclasts, as does calcitonin. The major factors that influence bone metabolism and their most important direct effects are listed in Table 50-1.
 |
PARATHYROID HORMONE
Although PTH was first shown to act directly on bone as a stimulator of resorption, much more is now known about its effects on osteoblasts at the cellular and molecular levels.14,30,31,32,33,34 and 35 Much of this information has been derived from investigations of isolated bone cells or cloned osteosarcoma cells that have an osteo-blastic phenotype, as well as from in vivo studies. The first effect of PTH on osteoblast-like cells is an activation of adenylate cyclase and protein kinase A. PTH can also accelerate phosphatidylinositol turnover, which leads to increased intracellular calcium and activation of protein kinase C. PTH causes rapid changes in osteoblast cell shape associated with polymerization of actin. A subsequent decrease in collagen synthesis is associated with a diminution of procollagen messenger RNA (mRNA) levels in the cell. Release of metalloproteinases from osteoblasts is also increased in response to PTH. Plasminogen activator activity is increased, in part by decreased production of an inhibitor, and this may result in the activation of latent collagenase. Alkaline phosphatase levels are usually decreased. PTH may also decrease BGP synthesis. PTH can increase prostaglandin synthesis and cell replication in bone cell and organ cultures.36
Most of these effects of PTH on bone can be considered catabolic; but prolonged, intermittent administration of low doses of PTH can elicit an anabolic effect, with increased bone mass.37 This is the basis for the use of intermittent PTH administration to treat osteoporosis. The anabolic response may be due to stimulation of precursor cell replication by PTH or release of growth factors from bone cells or matrix.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


