Menstrual disorders
Incidence %
A. DUB
381 (48.2 %)a
B. Amenorrhea
180 (22.8 %)
C. Oligomenorrhea
165 (20.9 %)
D. Dysmenorrhea
64 (8.1 %)
Total
790 cases
1.1 Dysfunctional Uterine Bleeding (DUB)
DUB (Table 1.1, A) is a painless endometrial bleeding that is prolonged, excessive, and irregular and not attributable to any underlying structural or systemic disease.
The etiology of DUB, during adolescence, arises out of continuing maturation of the hypothalamus [1–3]. In the USA the definition of DUB refers to anovulatory bleeding. The European Society of Human Reproduction and Embryology (ESHRE) defined DUB as excessive bleeding (excessively heavy, prolonged, or frequent) of uterine origin, which is not due to demonstrable pelvic disease, complication of pregnancy, or systemic disease. DUB can be either ovulatory or anovulatory [4].
A shift in the ratio of prostaglandins (PGs) and especially of the endometrial vasoconstrictor (PGF2a) to the vasodilator (PGE2) and an increase in total endometrial PGs have been demonstrated in ovulatory DUB patients [1, 5].
Diagnosis is made by the clinical history and the clinical examination, followed by the necessary laboratory tests, the pelvic ultrasonography, the endocrinological examination, and occasionally hysteroscopy and/or laparoscopy. DUB differential diagnosis includes pregnancy complications; neoplasms of the genital system; genital tract infections; endocrinopathies; treatment with various, several medications; trauma; coagulation disorders; and chronic systemic diseases.
The disease is classified in three groups as follows: group 1, mild hypermenorrhea (hemospherin (Hb) and hematocrit (Hct) within normal limits); group 2, moderate hypermenorrhea (Hb 9–10 g and no signs of anemia); and group 3, severe hypermenorrhea (Hb less than 8 g). The management depends on the severity of the disease and includes: the use of combined oral contraceptives (COCs,) progestogenic compounds followed by COCs, nonsteroidal anti-inflammatory drugs, transfusion, iron supplements, and reassurance [6–8].
1.2 Amenorrhea
Amenorrhea (Table 1.1, B) is classified as primary or secondary. Primary amenorrhea (PA) is the absence of menstruation in 16-year-old girls who have already developed secondary sexual characteristics or in 14-year-old girls who have no secondary sexual characteristics development. Especially for the second group, the term “late puberty” is preferable. Secondary amenorrhea (SA) is the absence of menstruation for 6 months. For adolescents with formerly regular cycles, SA is defined as the absence of menses for more than three subsequent periods [1, 5].
WHO classifies PA in three groups as follows: group I, no evidence of endogenous estrogen production, normal or low follicle stimulating hormone (FSH) levels, normal prolactin (PRL) levels, and no evidence of a lesion in the hypothalamic-pituitary region; group II, evidence of estrogen production and normal levels of PRL and FSH; and group III, which involves cases with elevated FSH serum levels indicating gonadal failure.
Table 1.2 presents the etiology of PA and SA.
Table 1.2
Etiology of PA or SA
1. Delayed puberty (PA) |
2. Congenital uterovaginal anomalies (PA or SA) |
3. Endocrine disorders (PA or SA) |
4. Premature ovarian failure (PA or SA) |
5. Chromosomal anomalies (PA or SA) |
6. Stress and psychological problems (PA or SA) |
Delayed puberty (DP) is presented as PA and is defined as the absence of onset of puberty by >2 SD later than the average age, i.e., >14 years in females [2, 8].
Congenital uterovaginal anomalies includes: obstruction of the genital tract and absence of the uterus or/and the vagina [9, 10].
Several endocrine disorders may also be the cause of PA or SA. Table 1.3 presents the causes of hypothalamic amenorrhea [2]. The pituitary causes of amenorrhea are: (a) Tumors: prolactinomas, other hormone-secreting pituitary tumors, nonfunctional tumors (craniopharyngioma) metastatic tumors. (b) Space-occupying lesions: empty sella syndrome, arterial aneurysm. (c) Pituitary necrosis: postpartum pituitary necrosis (Sheehan syndrome), panhypopituitarism, and systemic inflammatory diseases (sarcoidosis, hemochromatosis) [2, 8].
Table 1.3
 Management of Adolescent Hyperandrogenism
Management of Adolescent Hyperandrogenism
 Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Supplementation with DHEA in Poor Responder Patients
Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Supplementation with DHEA in Poor Responder Patients
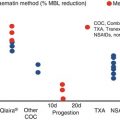 Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
 How to Choose the Right Contraceptive Method for the Right Woman
How to Choose the Right Contraceptive Method for the Right Woman
 Low Malignant Potential Tumors
Low Malignant Potential Tumors




Causes of hypothalamic amenorrhea
Related posts:
Management of Adolescent Hyperandrogenism
Polycystic Ovary Syndrome: From Contraception to Hormone Replacement Therapy
Supplementation with DHEA in Poor Responder Patients
Heavy Menstrual Bleeding: The Daily Challenge for Gynecologist
How to Choose the Right Contraceptive Method for the Right Woman
Low Malignant Potential Tumors
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
