Hemodialysis is one modality used to treat end-stage renal disease (ESRD) by filtering waste, removing extra fluid, and balancing and correcting electrolyte abnormalities and metabolic acidosis. ESRD patients most commonly undergo maintenance hemodialysis in outpatient centers multiple times a week. In 2017, there were more than 450 000 maintenance hemodialysis patients receiving care at some 6500 outpatient hemodialysis facilities.1 This represents about 88% of the ESRD population receiving renal replacement therapy (hemodialysis, peritoneal dialysis, or renal transplantation) in the United States. Approximately 1.8% of hemodialysis patients perform self or assisted therapy in their homes—that is, home hemodialysis. The ESRD program is administered by the Centers for Medicare and Medicaid Services (CMS) of the U.S. Department of Health and Human Services and is the only Medicare entitlement that is based on the diagnosis of a medical condition.
Maintenance hemodialysis patients are at increased risk for infection. Uremia is known to make patients with ESRD more susceptible to infectious agents through defects in cellular immunity, neutrophil function, and complement activation.2,3 In addition, for most maintenance hemodialysis patients, the process is performed several times per week in an environment where multiple patients receive hemodialysis concurrently, and requires vascular access, typically in the form of central venous catheter (CVC), arteriovenous fistula (AVF), or arteriovenous graft (AVG). As a result, repeated opportunities exist for acquisition and/or transmission of infection, via devices or through contaminated equipment, supplies, injectable medications, environmental surfaces, or hands of healthcare personnel (HCP).
Hemodialysis patients undergo frequent hospitalizations and surgery, which increase their opportunities for exposure and risk of developing healthcare-associated infections (HAIs). The annual adjusted mortality rate among hemodialysis patients is 167 per thousand patient-years at risk. Infection is the second leading cause of death in this patient population (accounting for ˜8% of all deaths)1 and is a likely contributor to many deaths attributed to cardiovascular causes. Not surprisingly, infections are also an important cause of hospitalization among hemodialysis patients. Rates of hospitalization due to cardiovascular and infectious causes are similar (46 vs 44 per hundred patient-years).4 Bacteremia (including that due to vascular access-related infections) and respiratory tract infections are common causes of hospitalization and death.5,6,7 In 2016, the number of hospital days due to infections for hemodialysis patients was more than twice that of patients who had received kidney transplants.4
This chapter describes (1) the major infectious diseases that can be acquired in the maintenance hemodialysis center setting; (2) important epidemiologic and environmental microbiologic considerations; and (3) infection prevention strategies. Many of the topics covered in this chapter focus on the outpatient in-center setting where maintenance hemodialysis currently most frequently occurs. However, many of these concepts may apply more broadly and be adapted to other settings where hemodialysis care is delivered, such as the acute care setting, long-term care facilities, or even patients’ homes.
BLOODSTREAM AND VASCULAR ACCESS INFECTIONS
Pathogenesis
Vascular access, specifically AVFs, AVGs, and CVCs, predisposes hemodialysis patients to bloodstream infections (BSIs) and other vascular access infections (VAIs). VAIs include BSIs that may be related to the dialysis vascular access and local infections at the site of the vascular access (eg, CVC exit site infection or tunnel infection). Bacterial or fungal pathogens causing such infections can either be endogenous (ie, caused by invasion of bacteria present in or on the patient) or exogenous (eg, acquired from contaminated dialysis fluids or equipment). CVC-related infections (a subset of VAIs) are most often caused by bacteria from the patient’s skin colonizing the outside of the catheter or from direct contact (eg, touch contamination by HCP) with the catheter hub, leading to contamination of the inner surface of the catheter.
Exogenous pathogens have caused numerous outbreaks, many of which resulted from inadequate dialyzer reprocessing procedures (eg, contaminated water or inadequate disinfectant concentration) or inadequate disinfection and maintenance of the water treatment and distribution system. Infections caused by endogenous pathogens tend to be more endemic and less frequently recognized as causing outbreaks.
Contaminated infusates or hematogenous spread are thought to be less common causes of BSIs, regardless of vascular access type. Contaminated medication vials have been reported in this setting. In 1999, an outbreak of Serratia liquefaciens BSIs and pyrogenic reactions among hemodialysis patients was traced to contamination of vials of erythropoietin.8 These vials, which were intended for single use, were contaminated by repeated puncture to obtain additional doses and by pooling of residual medication into a common vial.
Surveillance
Because of the importance of BSIs—particularly those related to the vascular access—in hemodialysis patients, the U.S. Centers for Disease Control and Prevention (CDC) initiated a voluntary ongoing surveillance system called the Dialysis Surveillance Network (DSN) in 1999.9 At the time, infections associated with hospital admission or intravenous (IV) antimicrobial receipt were included. This surveillance system was eventually expanded and has evolved into the Dialysis Event surveillance component of the National Healthcare Safety Network (NHSN).10 NHSN is the most widely used HAI surveillance system in the nation, with more than 25 000 facilities reporting HAI data to CDC via an internet-based system. Hemodialysis facilities report BSIs in dialysis patients and related events to NHSN’s Dialysis Event Surveillance. Outpatient hemodialysis facilities in the United States are eligible to participate and are instructed to follow a standard protocol,11 by which all outpatients who receive hemodialysis at the facility are monitored for three NHSN-defined dialysis events. The three types of dialysis events (positive blood culture; IV antimicrobial start; and pus, redness, or increased swelling at the vascular access site) are indicators of BSI and/or local vascular access site infection and are reported using a standard data collection form. Dialysis Event data reported to NHSN are used for dialysis facility performance measurement by CMS as part of the ESRD Quality Incentive Program (QIP)12; as a result, nearuniversal reporting to NHSN from outpatient hemodialysis facilities exists. In 2018, more than 6800 dialysis facilities reported 133,525 IV antimicrobial starts, 21,584 pus, redness, or increased swelling events at the vascular access site, and 24,736 positive blood cultures including 19,172 access-related positive blood cultures (CDC, unpublished data). A recognized challenge to complete BSI surveillance in this population is BSI diagnoses made in hospitals vs outpatient dialysis centers. Improved communication of such information from hospitals to outpatient dialysis centers and shared access to electronic health record data are potential solutions.13
Epidemiology and Risk Factors
Access site infections are particularly important because they can cause disseminated bacteremia or loss of the vascular access. Local signs of VAI include erythema, warmth, induration, swelling, tenderness, skin breakdown, loculated fluid, or purulent exudates.9,14,15,16 In 2018, the NHSN VAI pooled mean rate was 0.77 per 100 patient-months (CDC, unpublished data). The access-related BSI pooled mean rate was 0.36 per 100 patient-months, which varied by access type: 0.11 for fistulas, 0.24 for grafts, and 1.24 for CVCs (tunneled and nontunneled) (CDC, unpublished data). Rates of BSI, access-related BSI, and VAI are consistently and substantially higher among patients with CVCs compared to other vascular access types.
The primary risk factor for VAI is access type, with CVCs having highest risk for infection compared to AVGs and AVFs, which have substantially lower risk.9,14,15,16,17,18,19,20,21 An AVF is made by joining an artery and a vein typically in a patient’s arm where as an AVG uses a piece of tubing to join a patient’s artery and vein. Compared to native AVFs, the VAI risk is thought to be higher for AVGs; however, it is difficult to discern the increased risk specifically due to the AVG vs patient characteristics or other factors. Other potential risk factors for VAI include (1) location of the access in the lower extremity; (2) recent vascular access surgery; (3) trauma, hematoma, dermatitis, or scratching over the access site; (4) poor patient hygiene; (5) poor needle insertion technique; (6) older age; (7) diabetes; (8) immunosuppression; (9) iron overload; (10) IV injection; and (11) chronic inflammatory state.14,15,22,23,24,25,26,27
VAIs are caused (in descending order of frequency) by Staphylococcus aureus (32%-53% of cases), coagulase negative staphylococci (20%-32% of cases), gram-negative bacilli (10%-18%), other gram-positive cocci (including enterococci; 10%-12%), and fungi (<1%).18,19,28 Among BSIs, S aureus remains the most commonly reported pathogen (present in 31% of BSI and 32% of access-related BSI reported to NHSN); in 2014, 40% of the S aureus cultured from blood and with susceptibility information reported were resistant to methicillin.20
Based on the relative risk of both infectious and noninfectious complications, native AVFs are widely considered the preferred vascular access type; a goal of no more than 10% of patients maintained with permanent catheter-based hemodialysis treatment has been recommended.29,30,31,32 Data from Dialysis Outcomes and Practice Patterns Study (DOPPS) showed that from August 2010 to August 2013, AVF use increased from 63% to 68%, while catheter use declined from 19% to 15%.33 However, the majority of incident patients continue to initiate dialysis with a catheter. The 2018 and 2019 United States Renal Data System (USRDS) annual data reports showed that while 19.5% of prevalent (all) hemodialysis patients used a catheter, 80.1% of new patients started dialysis with a catheter, and there has been little change in the proportion of patients who initiate dialysis with a catheter over time.1,4 There are numerous barriers to performing permanent vascular access (ie, AVF or AVG) planning and placement in advance of dialysis initiation.34 For example, many patients lack pre-ESRD insurance because Medicare ESRD program benefits do not extend to individuals with late-stage chronic kidney disease (CKD), and a subset of patients who initiate dialysis in a hospital after experiencing a sudden decline in renal function may have had little opportunity for predialysis planning. Nonetheless, to minimize infectious complications, patients should ideally undergo early creation of a functional AVF, to minimize or eliminate the time dialyzed through a catheter.
Prevention
Recommendations for preventing VAIs have been developed by the CDC,35 its Healthcare Infection Control Practices Advisory Committee (HICPAC),36 and the National Kidney Foundation.29,30,31,32 CDC has developed a recommended “Approach to BSI Prevention in Dialysis Facilities” that includes core interventions to prevent BSIs among hemodialysis patients (Table 35-1). Facilities that implemented this set of interventions as part of a demonstration project were able to significantly reduce their access-related BSI rates and sustained these lowered rates for at least 4 years.37 The core interventions include (1) BSI surveillance and feedback of data to clinical staff; (2) hand hygiene observations and feedback (3) catheter/vascular access care observations and feedback; (4) development of staff infection prevention skills, demonstrated through competency assessments; (5) patient education and engagement in infection control processes; (6) efforts to decrease catheter prevalence; (7) use of alcohol-based chlorhexidine (>0.5%) as first-line skin antiseptic for CVC exit site care; (8) catheter hub disinfection; and (9) Polysporin triple ointment or povidone-iodine ointment (or potential alternatives) applied to catheter exit sites. CDC has also developed tools, protocols, and guidance to assist in the implementation of the interventions (https://www.cdc.gov/dialysis/prevention-tools/index.html).38
TABLE 35-1 Interventions for Dialysis Bloodstream Infection Prevention
Core interventions
Surveillance and feedback using NHSN
Conduct monthly surveillance for BSIs and other dialysis events using NHSN. Calculate facility rates and compare to rates in other NHSN facilities. Actively share results with front-line clinical staff.
Hand hygiene observations
Perform observations of hand hygiene opportunities monthly and share results with clinical staff.
Catheter/vascular access care observations
Perform observations of vascular access care and catheter accessing quarterly. Assess staff adherence to aseptic technique when connecting and disconnecting catheters and during dressing changes. Share results with clinical staff.
Staff education and competency
Train staff on infection control topics, including access care and aseptic technique. Perform competency evaluation for skills such as catheter care and accessing every 6-12 mo and upon hire.
Patient education/engagement
Provide standardized education to all patients on infection prevention topics including vascular access care, hand hygiene, risks related to catheter use, recognizing signs of infection, and instructions for access management when away from the dialysis unit.
Catheter reduction
Incorporate efforts (eg, through patient education, vascular access coordinator) to reduce catheters by identifying and addressing barriers to permanent vascular access placement and catheter removal.
Chlorhexidine for skin antisepsis
Use an alcohol-based chlorhexidine (>0.5%) solution as the first-line skin antiseptic agent for central line insertion and during dressing changes. Povidone-iodine (preferably with alcohol) or 70% alcohol are alternatives for patients with chlorhexidine intolerance.
Catheter hub disinfection
Scrub catheter hubs with an appropriate antiseptic after cap is removed and before accessing. Perform every time catheter is accessed or disconnected. If a closed needleless connector device is used, disinfect connector device per manufacturer’s instructions.
Antimicrobial ointment
Apply antibiotic ointment or povidone-iodine ointment to catheter exit sites during dressing change. Use of chlorhexidine-impregnated dressing might be an alternative.
BSI, Bloodstream infection; NHSN, National Healthcare Safety Network.
Adapted from https://www.cdc.gov/dialysis/prevention-tools/core-interventions.html
A large, cluster randomized trial lent further support to the CDC-recommended catheter care interventions.39 Specifically, consistent use of alcoholic chlorhexidine for CVC exit site care and alcohol for disinfection of the catheter hub (ie, scrub-the-hub) resulted in significant reductions in BSIs, antibiotic use, and hospitalizations for sepsis in CVC patients. Through the Making Dialysis Safer for Patients Coalition, CDC has partnered with a broad range of individuals and organizations, including professional organizations, dialysis delivery organizations, patient groups, health departments, certification organizations, and individual staff members and patients, and is working to educate dialysis providers, foster patient engagement, and facilitate implementation of the core interventions for BSI prevention.40,41
Multiple opportunities for hand hygiene exist during a single hemodialysis session and staff are frequently caring for more than one patient at a time. Hand hygiene practices of staff should be observed on a regular basis and feedback on performance provided to staff. A hand hygiene audit tool tailored for use in outpatient hemodialysis settings is available at https://www.cdc.gov/dialysis/prevention-tools/audit-tools.html as well as an educational brochure at https://www.cdc.gov/handhygiene/pdfs/Provider-Dialysis-Brochure-P.pdf (see also Chapter 4, Hand Hygiene).42,43
CDC recently updated the Guidelines for the Prevention of Intravascular Catheter-Related Infections to include recommendation for use of chlorhexidine-impregnated dressings to protect the insertion site of short-term, nontunneled CVCs in patients aged 18 years and older44 (https://www.cdc.gov/infectioncontrol/guidelines/bsi/c-i-dressings/recommendations.html). However, no recommendations were made for patients with long-term, tunneled catheters, which are far more common among maintenance hemodialysis patients. Few studies have specifically examined the use of chlorhexidine-impregnated dressings in hemodialysis patients with tunneled catheters and the effect of chlorhexidine-impregnated dressings on reducing catheter-related BSIs among hemodialysis patients remain largely unclear.45,46,47,48 Notably, several facilities that enrolled in the demonstration project evaluating CDC’s core interventions used chlorhexidine-impregnated dressings (disks) and were able to show sustained reductions in BSIs.37 Currently, CDC suggests the use of chlorhexidine-impregnated dressing as an alternative to antimicrobial ointment application to the exit site.
Other strategies that might assist in the implementation of recommended interventions include facilitating staff engagement and establishing safety culture within the facility. Use of a behavioral change strategy (“positive deviance”), in which strategies used by some staff members that achieve the desired outcome were encouraged among all staff, was shown to contribute to the reduction of BSI in one dialysis facility.49
Locking refers to the practice of instilling a solution into the catheter between dialysis sessions. There have been a number of studies that evaluated the efficacy of various antimicrobial locks (both antibiotic and nonantibiotic) in preventing catheter-related BSI among hemodialysis patients.50,51,52 Commonly studied antibiotic lock solutions in this population include vancomycin, gentamicin, and cephalosporins such as ceftazidime and cefazolin. Some examples of nonantibiotic lock solutions that have been studied in hemodialysis patients include taurolidine, methylene blue, and ethanol.53,54,55,56 Antimicrobials are typically combined with an anticoagulant such as citrate or heparin to maintain catheter patency. A recent Cochrane review concluded that antibiotic and combined (antibiotic and nonantibiotic) lock solutions decreased the incidence of catheter-related infections compared to control lock solutions, whereas nonantibiotic lock solutions reduced catheter-related infections only for tunneled catheters. However, confidence in the evidence was low and better-designed studies are needed to confirm the efficacy and safety of antimicrobial lock solutions.57 Currently, CDC and HICPAC guidelines recommend lock solutions in patients with multiple BSIs despite optimal adherence to aseptic technique.36 Routine prophylactic use of antimicrobial lock solutions for hemodialysis catheter-related BSIs is not recommended at this time and concerns remain about toxicities, antimicrobial resistance, and compounding of solutions in the outpatient setting. Currently there are no U.S. Food and Drug Administration (FDA)-approved nonantibiotic solutions for antimicrobial locks in hemodialysis patients, although some solutions are approved for use in other countries.58
A needleless connector (Tego® needlefree hemodialysis connector) was found to be significantly associated with less IV antibiotic use among hemodialysis patients; however, the risk of catheter-related BSI among patients who used the connector was not statistically significantly decreased.59 A recently developed catheter cap with a chlorhexidine gluconate-coated rod (ClearGuardTM HD) has been shown to reduce catheter-related BSIs and hospital admissions for BSI.60,61 The rod extends through the catheter hub and into the lumen releasing chlorhexidine into the lumen of the catheter. In one cluster-randomized, open-label trial, use of ClearGuardTM HD alone demonstrated significantly lower BSI rates than use of Tego® in combination with CurosTM (cap with 70% isopropyl alcohol).60 Given the evidence supporting the chlorhexidine-impregnated caps, this intervention could be considered particularly if BSI rates remain high in dialysis catheter patients, despite implementation of other routinely recommended measures.
Improving injection practices should be considered as a strategy to reduce both spread of bloodborne viruses (eg, hepatitis B and C) and BSIs.8 To reduce the risk of infection, medications should be prepared in an aseptic manner in a dedicated area and administered using aseptic technique as described in Table 35-2.62 Single use and multidose vials should be used according to manufacturer’s recommendations. CDC recommends (1) preparing medications in a separate room (preferred) or if a separate room is not available, in an area removed from the patient treatment area and designated for medications; (2) performing hand hygiene and using aseptic technique when preparing medication; (3) disinfecting the septum of the vial with alcohol and using a new needle and a new syringe to withdraw medication; (4) discarding single-dose vials after use and storing multidose vials appropriately; (5) not handling or storing used supplies, equipment, blood samples, or biohazard containers in or adjacent to areas where medications are handled; (6) delivering medications separately to each patient and not using common carts within the patient treatment area to prepare or distribute medications; and (7) performing hand hygiene, putting on new, clean gloves, scrubbing the injection port with antiseptic and using aseptic technique when administering medications.62 IV medication vials labeled for single use, including erythropoietin, should not be punctured more than once. Multidose medication vials should be assigned to a single patient whenever possible.64 An injection safety checklist and audit tool tailored for use in outpatient hemodialysis settings are available at https://www.cdc.gov/dialysis/prevention-tools/audit-tools.html.43
BLOODBORNE PATHOGENS
Hepatitis C
Hepatitis C virus (HCV) is moderately stable in the environment, and infectious virus can persist on surfaces when exposed to room temperature for at least 16 hours.65 Longer persistence of up to several weeks has been reported.66 HCV is most efficiently transmitted by direct percutaneous exposure to blood, and like hepatitis B virus (HBV), the chronically infected patient is central to the epidemiology of HCV transmission. HCV is not as efficiently transmitted as HBV in the dialysis setting. When recommended infection prevention practices (including basic injection safety) are implemented, these prevent HCV transmission among hemodialysis patients without the need for isolation.62,67,68,69 However, new acquisition of hepatitis C infection continues to occur among maintenance hemodialysis patients due to lapses in infection control. Currently, hepatitis C transmission occurs more commonly than hepatitis B spread in the dialysis setting. Patient-to-patient HCV spread likely occurs through blood contamination of items that are shared between patients without undergoing proper disinfection, such as medications, supplies, environmental surfaces, and/or HCP hands. The large, open floor plan in most dialysis clinics, rushed processes, and lack of physical barriers between patient treatment stations tends to facilitate lapses in hand hygiene and leads to poor separation between clean vs contaminated supplies.
TABLE 35-2 Recommended Infection Control Practices for Hemodialysis Units62
○ Before and after having direct contact with a patient’s intact skin
○ After contact with blood, body fluids or excretions, mucous membranes, nonintact skin, or wound dressings
○ After contact with inanimate objects (including medical equipment) in the immediate vicinity of the patient
○ If hands will be moving from a contaminated body site to a clean body site during patient care
○ After glove removal
Wear disposable gloves when caring for the patient or touching the patient’s equipment at the dialysis station; remove gloves and perform hand hygiene between each patient and station.
Items taken into the dialysis station should be disposed of or cleaned and disinfected before taken to a common clean area or used on another patient.
○ Nondisposable items taken to the patient treatment station that cannot be cleaned or disinfected (eg, adhesive tape) should be discarded after use.
○ Unused medications (including multidose vials) or supplies (syringes, alcohol swabs, etc.) taken to the patient’s station should be used only for that patient and should not be returned to a common clean area or used on other patients.
When multidose medication vials are used (including vials containing diluents), prepare individual patient doses in a clean (centralized) area away from dialysis stations and deliver separately to each patient. Do not carry multidose medication vials from station to station.
Do not use common medication carts to deliver medications to patients. Do not carry medication vials, syringes, alcohol swabs, or supplies in pockets.
Clean areas should be clearly designated for the preparation, handling, and storage of medications and unused supplies and equipment. Clean areas should be clearly separated from contaminated areas where used supplies and equipment are handled. Do not handle and store medications or clean supplies in the same or adjacent area to where used equipment or blood samples are handled.
Use external transducer protectors (venous or arterial) for each patient treatment to prevent blood contamination of the dialysis machine’s pressure monitoring equipment. Change these external transducer protectors between each patient treatment and when they become wet, and do not reuse them. The redundant internal transducer protectors do not need to be changed routinely between patients. If the external transducer protectors are contaminated with blood, the internal transducer protector should be assessed for contamination before dialyzing another patient with the same machine.
Clean and disinfect the dialysis station (chair, side tables, machine, IV pole, etc.) between patients.
○ Start cleaning only when patient has left the station and only admit new patient after cleaning and disinfection are complete.
○ Give special attention to cleaning control panels on the dialysis machine and other surfaces that are frequently touched and potentially contaminated with patient’s blood.
○ Discard all fluid, and clean and disinfect all surfaces and containers associated with the prime waste (including buckets attached to the machines). Allow prime buckets to air dry after disinfection and before use.
Do not reuse dialyzers or blood tubing. Place all used dialyzers and tubing in leak-proof containers for transport from station to reprocessing or disposal area.
Care of HBsAg-positive patients
Follow infection control practices recommended for all hemodialysis patients.
Dialyze HBsAg-positive patients in a separate room using separate machines, equipment, instruments, and supplies.
Staff members caring for HBsAg-positive patients should not care for HBV-susceptible patients at the same time (eg, during same shift or during patient change over).
Vaccinations
Hepatitis B vaccine
Vaccinate all susceptible patients against hepatitis B
Test for anti-HBs 1-2 mo after the last dose
○ If anti-HBs is <10 mIU/mL, consider patient susceptible, repeat the vaccine series, and retest for anti-HBs
○ If anti-HBs is ≥10 mIU/mL, consider immune and retest annually
▪ Give booster dose of vaccine if anti-HBs declines to <10 mIU/mL and continue to retest annually
Vaccinate all susceptible patient care staff, follow standard recommendations for post-vaccination testing of HCP Influenza vaccine
Annual vaccination for all patients
Annual vaccination for all staff
Pneumococcal vaccine
All patients should be vaccinated with pneumococcal vaccines per current guidelinesb
aAdapted from Centers for Disease Control and Prevention. Recommendations for preventing transmission of infections among chronic hemodialysis patients. MMWR Recomm Rep. 2001;50(RR-5):1-43.
bSchedule depends on the vaccination status of patients and is available on CDC Web site (https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/pneumo.html), Ref.63
HBsAg, hepatitis B surface antigen; anti-HBs, antibody to HBsAg.
Epidemiology In 2002, 63% of dialysis centers tested patients for antibody against HCV (anti-HCV).70 In the facilities that performed screening, the incidence rate in 2002 was 0.34%, and among these centers, the prevalence of anti-HCV among patients was 7.8%, a decrease of 26% since 1995. Only 11.5% of dialysis facilities reported newly acquired HCV infection among their patients. However, in other studies higher incidence rates have been reported from the United States (<1%-3%) and other countries [Japan (<2%), and Europe (3%-15%)].71,72,73,74,75,76,77,78 From 2012 to 2015, an overall HCV infection prevalence of 9.9% was reported among adult hemodialysis patients in high- and middle-income countries.79 Higher prevalence rates (10%->85%) also have been reported in individual facilities and in other countries.71,72,80,81,82,83,84
Hemodialysis patient- and facility-level risk factors associated with acquisition of HCV infection include blood transfusions from unscreened donors, transplantation of organs from donors with hepatitis C, injection drug use, high-risk sexual activity, low facility staff-to-patient ratio, time on dialysis, and receipt of dialysis in a facility with high HCV prevalence.76,77,78,85,86,87,88,89,90,91,92,93
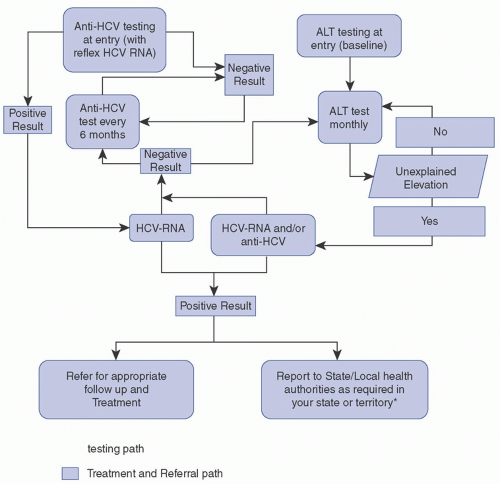
FIGURE 35-1 Hepatitis C screening algorithm. If the anti-HCV is positive, but the HCV RNA test is negative (eg, after treatment with a sustained virologic response), subsequent anti-HCV screening tests are replaced with HCV RNA testis. A change in HCV infection status (ie, new infection or seroconversion) should be reported to the state or local health department. ALT, alanine aminotransferase; anti-HCV, antibody to hepatitis C virus; HCV, hepatitis C virus; HCV-RNA, hepatitis C virus ribonucleic acid. (Reprinted from NTDS. Promoting Infection Prevention in Dialysis Facilities Hepatitis C Testing and Monitoring Algorithm. [cited December 31, 2019]. https://www.asn-online.org/g/blast/files/NCHHSTP_NTDS-HCV%20Subcommittee%20Algorithm_FINAL%2003.29.19.pdf, Ref.94)
Screening and Diagnostic Tests CDC recommends routine screening of maintenance hemodialysis patients for antibody to HCV (anti-HCV) on admission to the dialysis facility, and every 6 months thereafter for patients who test negative.62 For routine HCV screening of hemodialysis patients, the anti-HCV screening immunoassay (either rapid test or laboratory-based assay) is recommended. (Fig. 35-1, Table 35-3).95 FDA-licensed or approved tests to screen for anti-HCV in the United States do not discriminate between active and resolved HCV infection.96 All individuals who test anti-HCV positive should be further tested for HCV RNA by an FDA-approved nucleic acid test (NAT) to determine current infection status.95 In addition, monthly alanine aminotransferase (ALT) testing is recommended in all HCV-susceptible patients to detect increases in ALT that often occur before anti-HCV becomes positive. In recently updated guidelines from KDIGO (Kidney Diseases: Improving Global Outcomes), the organization recommends that HCV infection screening be conducted using NAT or immunoassay followed by NAT, if positive.97 KDIGO guidelines also suggest screening all patients upon initiation of peritoneal dialysis or home hemodialysis and recommend screening upon evaluation for kidney transplant. Although CDC, KDIGO, and other organizations recommend routine HCV screening of patients treated in hemodialysis facilities, this screening is not required nor reimbursed by CMS. As a result, incomplete detection and reporting of new cases across facilities is likely.
TABLE 35-3 Schedule for Routine Testing for Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV)
aResults of HBV testing should be known before patient begins dialysis, or as soon as possible after dialysis initiation.
bTest for HBsAg with an assay that can detect HBsAg mutants.
cNo ongoing HBV infection monitoring is recommended for patients with evidence of past, resolved infection. Screening for reappearance of HBsAg at regular intervals can be considered.
HBsAg, hepatitis B surface antigen; anti-HBs, antibody to HBsAg; HBcAg, anti-HBc, antibody to hepatitis B core antigen;
ALT, alanine aminotransferase; anti-HCV, antibody to hepatitis C virus.
Prevention of HCV Transmission Investigations of dialysis-associated outbreaks of hepatitis C infection indicate that HCV transmission most likely occurs because of inadequate infection prevention practices.98 CDC tracks HCV outbreaks in dialysis settings (https://www.cdc.gov/hepatitis/outbreaks/healthcarehepoutbreaktable.htm).99 From 2008 to 2018, 22 outbreaks involving at least 104 newly infected patients were reported to CDC. In those outbreaks, a common finding was that new infections occurred among patients receiving dialysis on the same machine immediately after or at stations adjacent to a chronically infected patient.100,101 Multiple opportunities for cross-contamination have been observed in the context of HCV transmission, including (1) shared equipment and supplies that were not disinfected between patient use; (2) use of common medication carts to prepare and distribute medications at patient stations; (3) sharing of multiple dose vials; (4) contaminated priming buckets that were not routinely changed or cleaned and disinfected between patients; (5) machine surfaces that were not routinely cleaned and disinfected between patients; and (6) blood spills that were not cleaned up promptly. In those outbreaks, a single common exposure event is rarely identified and many outbreaks involve separate chains of transmission occurring over time. Moreover, it has been noted that station turnover procedures (ie, process to prepare a dialysis treatment chair and machine for a next patient) are rushed, and disinfection of machine surfaces is initiated before the patient completing treatment has left the treatment station. These common practices are challenges to proper cleaning and disinfection of the machine and station to prevent cros-stransmission of bloodborne pathogens such as HCV.
Although incident HCV infection in a maintenance hemodialysis patient might represent acquisition through traditional HCV risk factors such as injection drug use, it is unknown how often traditional modes of transmission account for new cases in dialysis patients. When a new HCV infection ( including acute, symptomatic infection or HCV seroconversion) occurs in a dialysis patient, it should be assumed that the infection was healthcare-related and investigated as such, while also assessing other risk factors. State and local health departments to whom these infections should be reported have extensive expertise in evaluating traditional risk factors that the patient might have in addition to healthcare exposures. It is important to evaluate all healthcare exposures, including ones outside the dialysis facility, as potential contributors to HCV infection. In one investigation, a cluster of HCV infections among patients at a dialysis center was ultimately attributed to common exposure to procedures at a vascular access center.102 New HCV infection within a dialysis patient has also been attributed to receipt of dialysis (or other healthcare) during travel to developing countries.
The following recommendations can be applied to prevent transmission of HCV in dialysis facilities (https://emergency.cdc.gov/han/han00386.asp)103: (1) evaluate infection prevention practices in each facility and ensure adherence to infection control standards. CDC audit tools can be used to help assess practices such as injection medication preparation and administration, hand hygiene, and routine environmental surface cleaning and disinfection; (2) promptly address any identified gaps in infection prevention practices; (3) ensure dialysis staff are aware of and trained to implement infection prevention guidelines62; (4) follow CDC recommendations for HCV screening of hemodialysis patients and management of patients who test positive; and (5) immediately report any case of new HCV infection among patients undergoing hemodialysis to the state or local health department. Any new HCV infections among hemodialysis patients should be investigated.104
HCV-positive patients do not have to be isolated from other patients or dialyzed separately on dedicated machines.97 They should be referred for evaluation and treatment of HCV infection according to current medical practice guidelines. Treatment for HCV infection has substantially advanced in the past several years, and recent studies have shown that ESRD patients infected with HCV can be treated successfully.105,106 All dialysis patients with HCV infection should be referred for care and assessment for treatment. Since dialysis in a facility with high HCV prevalence is a risk factor for HCV infection, HCV treatment might help to decrease the number of new infections. As HCV elimination and micro-elimination efforts progress, more data on the impact of HCV treatment of hemodialysis patients may emerge.107
Hepatitis B
Epidemiology HBV is the most efficiently transmitted pathogen in the dialysis setting. During the early 1970s, HBV infection was endemic in maintenance hemodialysis units and outbreaks were common. Recommendations for control of hepatitis B in hemodialysis setting were first published in 1977,108 and by the 1980s, their widespread implementation was associated with a sharp decrease in the incidence of HBV infection among both patients and healthcare personnel (HCP).109,110 In 1982, the hepatitis B vaccine was recommended for all susceptible patients and HCP.111 Subsequently, the incidence and prevalence of HBV infection among maintenance hemodialysis patients in the United States declined dramatically, and by 2002, it was 0.12% and 1%, respectively.70 Data from 2002 showed that newly acquired HBV infections were reported by 2.8% of U.S. hemodialysis centers and 27.3% of centers reported one or more patients with chronic HBV infection.70
In past studies, independent risk factors among maintenance hemodialysis patients for acquiring HBV infection included the presence of ≥1 HBV-infected patient in the hemodialysis facility who was not isolated, as well as a vaccination rate <50% among patients in the facility.112 However, transmission has been rarely reported in the United States in the past 20 years due to high rates of vaccination, screening, and isolation. The segregation of HBsAg-positive patients and their equipment from HBV-susceptible patients resulted in 70%-80% reduction in the incidence of HBV infections among hemodialysis patients.110,113,114 Routine screening for markers of HBV infection, HBV vaccination of susceptible patients, and isolation of HBsAg-positive patients are all required by CMS.
HBV is transmitted by percutaneous (ie, puncture through the skin) or mucosal (direct contact with mucus membranes) exposure to infectious blood or body fluids that contain blood. HBV is relatively stable in the environment and has been shown to remain infectious for at least 7 days on environmental surfaces at room temperature.115,116,117 HBsAg has been detected in dialysis facilities on hemostats, scissors, dialysis machine control panels, and door knobs.117 HBV at titers of 102-103 virions/mL can be present on environmental surfaces in the absence of any visible blood and still cause infection.115,116,117,118 Thus, blood-contaminated surfaces that are not routinely cleaned and disinfected represent a means for HBV transmission. Dialysis HCP can transfer virus to susceptible patients from these environmental reservoirs, particularly when caring for multiple patients simultaneously.115,116,118
TABLE 35-4 Interpretation of Serological Test Results for Hepatitis B Virus Infection
eTransient HBsAg positivity might be detected in some patients following vaccination.
The most recent documented transmission in a dialysis clinic in the United States was due to reactivation of hepatitis B infection that occurred in a patient with previous infection who re-expressed surface antigen in the context of immunosuppression.119 CDC has received other reports of atypical hepatitis B serology results among dialysis patients that may represent reactivation of HBV infection or HBV mutant strains; however, no cases of dialysis-related transmission related to these instances have been identified.120,121
Other risk factors for acquiring HBV infection include injection drug use, sexual and household exposure to HBV-infected contacts, exposure to multiple sexual partners, male homosexual activity, and perinatal exposure.93 Dialysis patients with active HBV infection (HBsAg positive) should be educated about these and other risks. In these situations, sexual partners and household contacts should be informed and vaccinated.122,123,124 HBV-infected patients should be evaluated for HBV treatment.
Screening and Diagnostic Tests Several well-defined antigen-antibody systems are associated with HBV infection, including hepatitis B surface antigen (HBsAg) and antibody to HBsAg (anti-HBs); hepatitis B core antigen (HBcAg) and antibody to HBcAg (anti-HBc); and hepatitis B e antigen (HBeAg) and antibody to HBeAg (anti-HBe). Serologic assays are commercially available for all of these except for HBcAg because no free HBcAg circulates in the blood. One or more of these serologic markers are present during different phases of HBV infection and can help distinguish between acute or chronic infection (Table 35-4).125 HBV infection can also be detected, using qualitative or quantitative tests for HBV DNA.126,127 These tests are most commonly used for HBV-infected patients being managed with antiviral therapy.128,129,130,131,132 HBV DNA testing can also be valuable to evaluate the possibility of hepatitis B reactivation and when infection with HBV mutant strains is suspected.120,121 Recommendations for routine testing for HBV in maintenance hemodialysis patients are described in Table 35-3.
The presence of HBsAg usually correlates with viremia (positive HBV DNA) and is indicative of ongoing HBV infection and potential infectiousness. In newly infected individuals, HBsAg is present in serum on average 30 days (range 6-60 days) after exposure to HBV and persists for variable periods. Anti-HBc develops in all HBV infections and persists for life. Acute or recently acquired infection can be distinguished by presence of the immunoglobulin M (IgM) class of anti-HBc, which persists for ˜6 months. In individuals who recover from HBV infection, HBsAg and HBV DNA are usually eliminated from the blood and anti-HBs appears. After recovery from natural infection, most individuals will be positive for both total anti-HBc and anti-HBs, whereas only anti-HBs develops in individuals who are successfully vaccinated. Most individuals who do not recover and remain chronically infected remain HBsAg, total anti-HBc, and HBV DNA positive. HBeAg can be detected in acute or chronic HBV infection and usually correlates with viral replication and high-level viremia (ie, high infectivity) while anti-HBe correlates with loss of replicating virus and lower levels of virus. All HBsAg-positive patients are potentially infectious. Patients’ HBsAg status should be determined upon admission to (or first treatment within) a dialysis unit, and HBsAg-positive patients should be isolated. Because of the potentially serious consequences of missing an individual with HBV infection in a dialysis center, dialysis providers should routinely use HBsAg assays that are capable of detecting common HBV mutant strains.120,121
In some individuals, the only HBV serologic marker detected is total anti-HBc (ie, isolated anti-HBc). Among most asymptomatic persons in the United States tested for HBV infection, an average of 2% (range: <0.1%-6%) test positive for anti-HBc133; among injection drug users, however, the rate is 24%-28%.134,135 This pattern can occur after HBV infection among individuals who have recovered but whose anti-HBs have waned or among individuals who have low-level chronic HBV infection and failed to develop anti-HBs. It may also represent a false-positive total anti-HBc result or someone in the early convalescent period after natural infection before the appearance of anti-HBs. HBV DNA has been detected in <10% of individuals with isolated anti-HBc, and these individuals are unlikely to be infectious to others except under unusual circumstances involving direct percutaneous exposures to large quantities of blood (eg, transfusion) or organ transplantation.134,135,136,137,138,139 However, the rare individual with high titers of HBV DNA and isolated anti-HBc is likely infectious, even if HBsAg negative, and should be dialyzed in isolation while diagnostic workup proceeds with expert consultation.120 In most persons with isolated anti-HBc in the general population, the result appears to be false positive. Data from several studies have demonstrated that a primary anti-HBs response develops in most of these individuals after a three dose series of hepatitis B vaccine.140,141 No data exist on response to vaccination among hemodialysis patients with this serologic pattern. Testing and follow-up recommendations for hemodialysis patients with isolated anti-HBc are available.62
Only gold members can continue reading. Log In or Register to continue
 Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
 Healthcare-Associated Infections Related to the Use of Intravascular Devices
Healthcare-Associated Infections Related to the Use of Intravascular Devices
 MDRO Infections: Gram-Positive Organisms (Including Methicillin-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococcus)
MDRO Infections: Gram-Positive Organisms (Including Methicillin-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococcus)
 Epidemiology and Prevention of Healthcare-Associated Infections Related to Animals in the Hospital
Epidemiology and Prevention of Healthcare-Associated Infections Related to Animals in the Hospital



