Fig. 10.1
PRISMA 2009 Flow Diagram for systematic review of publications since 2006, when the last review was undertaken
Descriptive Data Synthesis
Table 10.1 presents study characteristics of 34 studies included for review, which were published in years ranging from 2005 to 2015 [25–60]. Studies were heterogeneous for age, ethnicity and screening/diagnostic characteristics. For instance, case definition of diabetes using HbA1c diagnostic cutoffs was varied across studies between ≥6.5 and >7.0 %, and from 5.7–6.4 % to >6.0 % for pre-diabetes (Table 10.1). Only one study used the oral glucose tolerance test (OGTT) in a population-based sample [57]. Similarly, pre-existing diabetes has been identified through self-report, primary care/general practice records, hospital chart review and data linkage between pharmaceuticals and/or laboratory investigations and hospital admissions/national administrative datasets. Study populations were identified/recruited using various methods including community screening, clinic databases and population based health databases (Table 10.1).
Table 10.1
Characteristics of observational studies reviewed
Study identification | Study design (follow-up) | Participants and setting | Outcomes (measures, units) |
|---|---|---|---|
Agban et al. (2008) [25] | Cross-sectional (baseline and 2 years from cohort study) | Sample size: N = 7782 Age (years): range in mean from 56 to 68 Gender: male 42 % Ethnicity: European, Māori, Pacific, Asian (Indian), other Asian, Other (Middle Eastern, Latin American/Hispanic and African) Eligibility criteria: T2D patients who had undertaken an annual review in 2002 or 2003, and had a follow-up review 2 years later Setting: nationwide data from primary health care reviews of patients with T2D collated within 15 primary care organisations or diabetes trusts | Baseline and 2 years for all outcomes Poor glycaemic control prevalence (HbA1c >8 %, %) HBP prevalence (>130/80, %) Obesity prevalence (measured BMI ≥30 for European, Asian, Indian and ‘Other’; BMI ≥32 for Māori and Pacific, %) Current smoker prevalence (self-report, %), |
Brian et al. (2010) [26] | Population-based cross-sectional survey using multistage cluster random sampling | Sample size: N = 1381 (73 %) Age (years): ≥40 Gender: NR Ethnicity: Fijian Eligibility criteria: HbA1c and visual acuity were measured Setting: Diabetic eye disease was assessed using 90-dioptre lens dilated funduscopy | HbA1c and visual acuity measured Mean HbA1c (9.9 ± 2.3 %) Vision threat occurred in at least one eye of 11.5 %. Diabetes (predominantly maculopathy) caused pinhole acuity <6/18, <6/60 and <3/60 for 3.8 %, 1.1 % and 0.7 % of eyes, respectively. No person was bilaterally blind (<6/60) due to diabetes, but 2.3 % (all on oral antiglycaemics alone) were 6/60 bilaterally. Compared with recent diabetes diagnosis, diagnosis >10 years ago was predictive of any (odds ratio [OR] 8.13; 95 % confidence interval [CI] 3.28–20.21; P < 0.001) and vision-threatening (OR 5.25; 95 % CI 1.71–16.12; P = 0.004) eye disease. Although 80.6 % claimed regular general diabetes checkups, only 36.5 % recalled previous dilated ocular examination. Four eyes had received laser treatment |
Brewer et al. (2008) [27] | Cross-sectional (baseline from cohort study) and prospective cohort and (median 2 years) | Sample size: N = 47,904 (408 with prior diagnosis of diabetes) Age (years): ≥0 Gender: male 44 % Ethnicity: European/other, Māori, Pacific, Asian (unspecified) Eligibility criteria: participants in a Hepatitis Foundation screening campaign for hepatitis B (1999–2001) Setting: lower half of the North Island of NZ | Diabetes prevalence (HbA1c ≥7 %, %) All-cause mortality (data linkage, HR with 95 % CI) |
Chan et al. (2015) [28] | Retrospective cohort (from 2004 to 2010) | Sample size: N = 1,475,347 Age (years): ≥0 Gender: male 48 % Ethnicity: European/other, Māori, Pacific, Asian (Indian), Chinese, other Asian Eligibility criteria: residents who had utilised publicly funded health services in NZ and lived in Auckland in 2010 Setting: Auckland metropolitan region, linked data between a laboratory repository and national administrative datasets for District Health Boards | Age-standardised diabetes prevalence (dysglycaemia by modified ADA and WHO criteria, %) |
Coppell et al. (2013) [29] | Cross-sectional | Sample size: N = 4721 Age (years): ≥15 Gender: NR Eligibility criteria: NR Ethnicity: European/Other (Asian, Middle Eastern, Latin American and African), Māori, Pacific Setting: nationwide, 2008/2009 New Zealand Adult Nutrition Survey | Diabetes prevalence (self-report diagnosed or HbA1c ≥6.5 %, %) Pre-diabetes prevalence (HbA1c 5.7–6.4 %, %) |
Elley et al. (2008) [30] | Cross-sectional | Sample size: N = 29,179 Age (years): range in mean from 56 to 68 Gender: NR Eligibility criteria: T2D Ethnicity: European, Māori, Pacific, Asian (Indian), Other Asian, Other Setting: nationwide linked hospital records and data obtained from primary health care reviews of patients with T2D | Poor glycaemic control prevalence (HbA1c >8 %, %) HBP prevalence (>130/80, %) Obesity prevalence (measured BMI ≥30, %) Albuminuria prevalence (ACR ≥2.5 for men; ≥3.5 for women, %) Current smoker (self-report, %), 5-year CVD risk prevalence (Framingham risk score ≥15 %, %) |
Elley et al. (2010) [31] | Prospective cohort (median 3.9 years) | Sample size: N = 36,127 Age (years): median 59 Gender: male 49 % Eligibility criteria: T2D without previous CVD Ethnicity: European, Māori, Pacific, Asian (Indian), East Asian, Other (Middle Eastern, Latin American/Hispanic, African, and others) Setting: nationwide linked hospital records and data obtained from primary health care reviews of patients with T2D | Fatal or nonfatal CVD incidence (data linkage using ICD-9 and ICD-10 codes, HR with 95 %CI) |
Ellison et al. (2005) [32] | Cross-sectional | Sample size: N = 50,819 Age (years): >20 Gender: male 44.6 % Ethnicity: European, Māori, Samoan, Cook Island, Asian (Indian), Chinese Eligibility criteria: none specified Setting: South Auckland. Screening programme to detect elevated fasting hyperglycaemia using HbA1c | Diabetes prevalence (HbA1c >7 %, %) Pre-diabetes or diabetes prevalence (HbA1c >6 %, %) |
Faatoese et al. (2011) [33] | Cross-sectional | Sample size: N = 252 Age (years): range 20–64 Gender: male 40 % Ethnicity: Māori Eligibility criteria: Māori descent Setting: community screening for CVD risk factors in Wairoa | T2D prevalence (prior diagnosis by medical records, %) |
Feigin et al. (2006) [34] | Cross-sectional | Sample size: N = 1423 Age (years): ≥15 Gender: Male 47 % Ethnicity: European, Māori/Pacific, Asian/other (unspecified) Eligibility criteria: first-ever cases of stroke 2002–2003 Setting: Auckland population-based register | Diabetes (doctor diagnosed by self-report, %) |
Frederikson and Jacobs (2008) [35] | Cross-sectional (baseline from cohort study) | Sample size: N = 11,977 Age (years): range 7–100 Gender: Male 52 % Ethnicity: European, Māori, Pacific (Samoan, Cook Island Māori, Tongan, Niuean), Asian (Indian), Chinese, Other Eligibility criteria: all records of first screening visits 2002–2005 for people with diabetes Setting: Wellington regional retinal screening programme for people with diabetes | Maculopathy prevalence (clinical retinopathy screening, %) |
Grey et al. [36] | Cross-sectional | Sample size: N = 10,301 Age (years): range 35–74 Gender: male 52 % Ethnicity: Pacific (Samoans, Tongan, Cook Island Māori, Niuean) Other Pacific (including Tokelauan) Eligibility criteria: none specified (Fijian excluded) Setting: primary care practices in nine Primary Health Organisations in Auckland and Northland | Diabetes prevalence (electronic medical records, %) |
Ihaka et al. (2012) [37] | Cross-sectional | Sample size: N = 53 Age (years): ≥18 Gender: men 53 % Ethnicity: Māori Eligibility criteria: Māori with diabetes who had not received a national diabetes assessment for >12 months and had undetected pedal pulses, absence of sensation, previous history of peripheral vascular disease, or ulceration and no below-knee amputation Setting: Waitemata district, Auckland 2007–2008 | Classification of foot risk status (podiatric practitioners category ≥2, %) Obesity, hypertension, dyslipidaemia and retinopathy prevalence (self-report, %) |
Jackson et al. (2009) [38] | Retrospective cohort (from 1996 to 2007) | Sample size: N = 45,970 Age (years): ≥0 Gender: NR Ethnicity: European/other, Māori, Pacific, Asian (Indian), Chinese, Other Asian Eligibility criteria: public hospital discharge with any mention of T1D or T2D from 1996 to 2007 Setting: counties Manukau National Minimum Dataset, 2007 | Hospital admissions for people with diagnosed diabetes (hospital records, %) |
Jeffreys et al. (2005) [39] | Prospective cohort (13 years) | Sample size: N = 74,847 Age (years): ≥25 Gender: male 50 % Ethnicity: European/other (non-Māori/non-Pacific), Māori, Pacific Eligibility criteria: hospital discharge diagnosis of diabetes between 1988 and 2001 Setting: record linkage study of national hospital discharge records to death records | All-cause mortality (data linkage hospital discharge to death records, %) |
Joshy et al. (2009) [40] | Retrospective cohort (from 2003 to 2006) | Sample size: N = 7900 Age (years): NR Gender: male % NR Ethnicity: European, Māori Eligibility criteria: renal complication-free adult diabetes patients registered with Waikato regional diabetes service, diagnosed with diabetes before 2003 Setting: Waikato District Health Board region | Hospital renal admission (hospital records, HR with 95 % CI) Start dialysis or kidney transplantation (hospital records, HR with 95 % CI) Death from renal disease (data linkage to death records, HR with 95 % CI) |
Joshy et al. (2009) [41] | Cross-sectional | Sample size: N = 45,500 Age (years): NR Gender: Male % NR Ethnicity: European, Māori, Pacific, Asian Eligibility criteria: all patients registered with the practices as of 1 July 2007 Setting: 10 Rotorua General Practice Group practices | Age-standardised diabetes prevalence (medical records, %) |
Joshy et al. (2009) [42] | Cross-sectional | Sample size: N = 1819 Age (years): ≥18 Gender: Male 49 % Ethnicity: European, Māori, Pacific, Asian Eligibility criteria: all patients with diabetes registered with the practices as of 1 July 2007 Setting: 10 Rotorua General Practice Group practices | CKD prevalence (eGFR<60, %) Microalbuminuria prevalence (ACR 2.5–29.9 for men; 3.5–29.9 for women, %) Albuminuria prevalence (ACR ≥30, %) |
Joshy et al. (2010) [43] | Retrospective cohort (from 2003 to 2007) | Sample size: N = 9043 Age (years): ≥18 Gender: male 50 % Ethnicity: European, Māori Eligibility criteria: diabetes patients registered with the Waikato Regional Diabetes Service database before 2008, diagnosed before 2003 and alive as of 2003 Setting: Waikato region | Age-standardised, all-cause mortality rate (data linkage,/100,000 person-years) |
Kenealy et al. (2008) [44] | Cross-sectional (baseline from cohort) and prospective cohort (median 2.4 years) | Sample size: N = 48,444 Age (years): range in mean 53–66 Gender: male 49 % Ethnicity: European, Māori, Pacific, Asian (Indian), East Asian, Other (Middle Eastern, Latin American/Hispanic, African, others) Eligibility criteria: T2D and no previous CVD Setting: people with T2D who attended at least one diabetes annual review in primary health care as part of a national programme from 2000 to 2005; forms the NZ Diabetes Cohort Study | Fatal/nonfatal CVD incidence (data linkage to hospital/mortality data, HR with 95 %) Microalbuminuria prevalence (ACR ≥2.5 for men; ≥3.5 for women, %) Macroalbuminuria prevalence (ACR >30, %) Current smoker prevalence (self-report, %) Poor glycaemic control prevalence (HbA1c ≥10 %, %) |
Kenealy et al. (2012) [45] | Cross-sectional | Sample size: 65,171 Age (years): median 65 Gender: male 51 % Ethnicity: European, Māori, Pacific, Asian (Indian), East Asian, Other (Middle Eastern, Latin American/Hispanic, African, others) Eligibility criteria: adults in primary care with T2D, not on renal replacement therapy Setting: T2D who had attended at least one diabetes annual review in primary health care as part of a national programme between 2000 and 2006 in New Zealand; forms the NZ Diabetes Cohort Study | Microalbuminuria prevalence (ACR >2.5 men, 3.5 women to <30, %) Macroalbuninuria prevalence (ACR 30–<100, %) Advanced albuminuria prevalence (ACR ≥100, %) |
Kerr et al. (2006) [46] | Cross-sectional (baseline from cohort) and prospective cohort (mean 3.8 years) | Sample size: N = 4193 Age (years): range in mean 55–60 Gender: Male 49 % Ethnicity: European, Māori, Pacific, Asian, Other Eligibility criteria: T2D Hospital admission for MI or CCF from 1999 to 2001 Setting: the study population included 4193 individuals with T2D from South Auckland who participated in a primary care audit from 1994 to 1999 | Mortality (data linkage, HR with 95% CI) Smoking prevalence (self-report, %) |
Kerr et al. (2008) [47] | Cross-sectional | Sample size: N = 973 Age (years): mean 60 Gender: Male 75 % Ethnicity: European/other, Māori, Pacific, Asian Eligibility criteria: patients admitted for acute CV event Setting: patients presenting to Middlemore Hospital Coronary Care Unit with an acute CVD event from July 2004 to June 2006. CVD risk factor data was electronically collected using acute PREDICT | T2D prevalence (diagnosed, %) |
Kolt et al. (2007) [48] | Cross-sectional | Sample size: 112 Age (years): mean 66 Gender: male 45 % Ethnicity: Asian (India, Sri Lanka, Pakistan, Fiji) Eligibility criteria: NR Setting: Auckland-based Asian Indian community organisations | Diabetes prevalence (self-report, %) |
Lawrenson et al. (2009) [49] | Cross-sectional | Sample size: N = 26,096 Age (years): ≥20 Gender: NR Ethnicity: European, Māori, Asian Eligibility criteria: aged ≥20 years with T2D Setting: Hamilton general practice register linked to Waikato regional diabetes service register | Poor glycaemic control prevalence (HbA1c >8 %, OR with 95% CI) |
Lim et al. (2008) [50] | Cross-sectional | Sample size: 180 Age (years): mean 54 Gender: male 44 % Ethnicity: Māori Eligibility criteria: household members with at least one Māori resident, or Māori with past GDM or aged ≥23 years with 2 parents with known diabetes Setting: newly diagnosed with diabetes during a community screening programme, Te Wai o Rona Diabetes Prevention Strategy | Poor glycaemic control prevalence (HbA1c ≥8.0 %, %) HBP prevalence (treated hypertension or ≥130/85, %) Central obesity prevalence (waist circumference >102 cm for men, >88 cm for women, %) Metabolic syndrome prevalence, (ATPIII criteria, %) Current prevalence (self-report, %) Microalbuminuria prevalence (ACR 2.5–29.9 for men, 3.5–29.9 for women, %) Albuminuria prevalence (ACR ≥30, %) CKD prevalence (eGFR <60, %) Retinopathy prevalence (microaneurysms ≥5, %) |
New Zealand Ministry of Health (2013/2014) [51] | Cross-sectional | Sample size: N = 13,309 Age (years): ≥15 Gender: men and women, the proportion is not noted Eligibility criteria: resident population aged ≥15 years living in permanent dwellings, aged-care facilities or student accommodation Ethnicity: European/Other, Māori, Pacific, Asian Setting: nationwide, New Zealand Health Survey | Diabetes prevalence (self-report, adjusted rate ratios [for age, gender, ethnicity]) |
Robinson et al. (2006) [52] | Cross-sectional | Sample size: 5917 Age (years): mean 60 Gender: male 50 % Ethnicity: European, Māori, Pacific, Asian (Indian), Other Asian, Other Eligibility criteria: patients with diabetes Setting: external audit of general practice diabetes care carried out in South and West Auckland by the Diabetes Care Support Service | Poor glycaemic control prevalence (HbA1c >8.0 %, %) Albuminuria prevalence (ACR ≥2.5 for men; ≥3.5 for women, %) Current smoker prevalence (self-report, %) Obesity prevalence (BMI >30, %) HBP prevalence (systolic >140, %) At-risk feet (by clinical review, %) Dyslipidaemia prevalence (TC:HDL ratio>4.5) |
Robinson et al. (2015) [53] | Cross-sectional (baseline from cohort) and prospective cohort (median 7.14 years) | Sample size: N = 62,002 Age (years): range in mean 55–66 Gender: male 49 % Ethnicity: European/other, Māori, Pacific, Asian (Indian subcontinent or Fijian Indians), other Asian (Southeast Asian, Chinese) Eligibility criteria: T2D Setting: nationwide | Microalbuminuria prevalence (ACR ≥2.5 for men or ≥ 3.5 for women, and < 30 for both, %) Macroalbuminuria prevalence (ACR ≥30, %) Lower limb amputation incidence (linked hospital records ICD codes, rate/1000 person years) |
Scott et al. (2006) [54] | Cross-sectional | Sample size: 1251 Age (years): <26 Gender: male 50 % Ethnicity: Māori/Pacific Islanders, Europeans, Others Eligibility criteria: attended a diabetes centre at least once in the previous 3 years, any person with diabetes born after 1 January 1978 Setting: 12 paediatric hospital and adult hospitals across NZ and forms the all-NZ young person’s diabetes audit, 2003–2004 | Microalbuminuria prevalence (ACR >2.5 for males; >3.5 for females, %) |
Scott et al. (2007) [55] | Cross-sectional (baseline from retrospective cohort) | Sample size: 4408 Age (years): mean 68 Gender: male 65 % Ethnicity: European, Māori Eligibility criteria: hospital discharge diagnosis of all with acute coronary syndromes from 1999 to 2002 Setting: Waikato hospital, Hamilton | Diabetes prevalence (chart review, %) |
Scott et al. (2008) [56] | Cross-sectional | Sample size: N = 12,992 Age (years): ≥16 Gender: male 41 % Ethnicity: European/other, Māori, Pacific Eligibility criteria: subsample with any 12-month mood and anxiety disorder prevalence (CIDI 3.0/DSM-IV) for diabetes prevalence and subsample with diabetes for mental disorder prevalence Setting: nationwide | Diabetes prevalence (self-report, %) Any 12-month mood and anxiety disorder prevalence (CIDI 3.0/DSM-IV, %) |
Simmons et al. (2009) [57] | Cross-sectional | Sample size: 3784 Age (years): ≥28 Gender: male 36 % Ethnicity: Māori Eligibility criteria: nonpregnant adult Māori Setting: all Māori residents within the boundaries of the Waikato District Health Board and the tribal area of Ngati Tuwharetoa in the neighbouring Lakes District Health Board | Undiagnosed diabetes, IGT, and IFG age-standardised prevalence (OGTT 1998 WHO criteria, % with 95 %CI) |
Smith et al. (2010) [58] | Cross-sectional | Sample size: 1.4 million Age (years): ≥0 Gender: male 46 % Ethnicity: European/other, Māori, Pacific, Asian Eligibility criteria: health events recorded between January 2006 and December 2007 for those alive Setting: records of subsidy claims for pharmaceuticals and laboratory investigations were linked to records in a national hospital admissions database to ‘reconstruct’ populations of four District Health Boards – Counties Manukau, Northland, Waitemata and Auckland | Diabetes age-standardised prevalence (data linkage records ICD-10-AM system, %) Age-standardised proportion of diabetes cases ≥1 medical/surgical hospital admissions in 2007 (data linkage records, %) |
Tomlin et al. (2006) [59] | Cross-sectional | Sample size: 13,281 Age (years): ≥0 Gender: Male 52 % Ethnicity: European, Māori/Pacific Eligibility criteria: any diabetes Setting: data were collected from all 242 practices participating in the South Link Get Checked programme, every practice in the South Island outside Christchurch city (the main urban centre) and 14 practices within Christchurch | Poor glycaemic control prevalence (HbA1c >9.0 %, %) Microalbuminuria prevalence (ACR >2.5 for males; >3.5 for females, %) High Cholesterol prevalence (≥6.0, %) Smoking prevalence (self-report, %) |
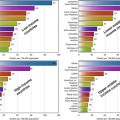
Table 10.2 shows the prevalence of diabetes and pre-diabetes. The prevalence of known diabetes was estimated to be 2.2–5.0 % among Europeans vs. 7.0–12.2 % among Māori, 8.9–38 % among Pacific people and 9.1–37.1 % among Asians. The prevalence of diabetes including known diabetes and undiagnosed diabetes by HbA1c screening ranged from 1.1 to 6.1 % among Europeans but 3.3 to 9.8 % among Māori, 5.3–15.4 % among Pacific peoples and 4.3–9.3 % among Asians. Undiagnosed diabetes alone ranged from 0.4 to 1.1 % among Europeans but 3.6–6.5 % among Māori, 4.6–8.1 % among Pacific people and 7.4–7.5 % among Asians. No consistent gender differences were found.
Table 10.2
Prevalence of diabetes and pre-diabetes
Gender | European | Māori | Pacific | Asian | |
|---|---|---|---|---|---|
Diabetes prevalence and key features | |||||
Brewer et al. (2008) [27] HbA1c screening/prior diagnosis; age 56–68 years | 1.1 | 3.3 | 5.3 | 4.3 | |
Chan et al. (2015) [28]a Prior diagnosis; age 0+ years | Male | 3.0 | 8.2 | 11.4 | 10.8 |
Female | 2.2 | 7.0 | 11.6 | 9.3 | |
Coppell et al. (2013) [29] HbA1c screening/prior diagnosis; age 15+ years | 6.1 | 9.8 | 15.4 | ||
Ellison et al. (2005) [32]a
Related posts: Diabetes in Indigenous Australians and Other Underserved Communities in Australia Diabetes in Indigenous Australians and Other Underserved Communities in Australia
 Diabetes in Ethnic Minorities and Immigrant Populations in Western Europe Diabetes in Ethnic Minorities and Immigrant Populations in Western Europe
 Diabetes Among Indigenous Canadians Diabetes Among Indigenous Canadians
 Type 2 Diabetes in the Middle East and North Africa (MENA) Type 2 Diabetes in the Middle East and North Africa (MENA)
 Primary Prevention of Type 2 Diabetes: An Imperative for Developing Countries Primary Prevention of Type 2 Diabetes: An Imperative for Developing Countries
 Diabetes in China and the Western Pacific Region Diabetes in China and the Western Pacific Region
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| |||||