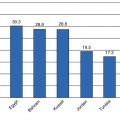
Fig. 13.1
Prevalence of self-reported diabetes among Indigenous peoples aged 12 years and older, Canada, 2006, 2008–2010, 2009–2010 (Source: Public Health Agency of Canada (2011), using data from 2009 to 2010 Canadian Community Health Survey (Statistics Canada); First Nations Information Governance Centre (2011), using data from the 2008–2010 First Nations Regional Longitudinal Health Survey (Phase 2) (First Nations Information Governance Centre); Social and Aboriginal Statistics Division, Aboriginal Peoples Survey, 2006: Inuit Health and Social Conditions: Ottawa, ON: Statistics Canada; 2008. Statistics Canada. Public Health Agency of Canada. 2011)
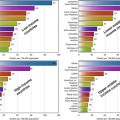
Administrative data from Manitoba reported a prevalence rate of type 2 DM that was 4.5 times higher than that in the non-First Nation population of Manitoba [22]. Similarly, a study in Saskatchewan also using administrative data showed that the prevalence of diabetes was four times higher among First Nations women than among non-First Nations women and 2.5 times higher among First Nations men than non-First Nations men (Fig. 13.2) [23]. According to administrative data from 2007, the prevalence of diabetes was 13.5 % in Indigenous peoples compared to 6 % in non-Indigenous peoples in the province of Alberta [24].
Fig. 13.2
Age-standardized diabetes prevalence in First Nations and non-First Nations men and women from 1990 to 2005 (Dyck et al. [23])
Over the past three decades, a limited number of more detailed studies using standardized oral glucose tolerance tests (OGTTs) have reported prevalence rates in Indigenous Canadians to be among the highest in the world (Fig. 13.3) [25, 26]. High prevalence rates were found in two Quebec communities, with a 48.6 % prevalence rate in Algonquin women of Lac Simon (aged 15 years and older) and a 16.3 % prevalence in women of River Desert (aged 15 years and older) [26]. According to a study in Sandy Lake First Nation, the age-standardized prevalence of type 2 DM was 26.1 % [25] over the age of 10.
Fig. 13.3
Age- and sex-specific prevalence of impaired glucose intolerance, newly diagnosed diabetes, and previously diagnosed diabetes in Sandy Lake First Nation (Harris et al. [25])
Although the administrative data studies mentioned above have presented both incidence and prevalence rates of type 2 DM [22, 23], there are still relatively limited data on incidence of type 2 DM in Indigenous populations [23, 24]. In the Indigenous population of Alberta, the incidence of diabetes during 1995–2007 increased at a slower rate compared to the general population, even though the overall rates were higher among Indigenous people [24]. There has been one follow-up study using repeat OGTTs, which reported a 17 % diabetes conversion rate over 10 years [27].
In contrast to First Nations, data on diabetes prevalence and incidence among Métis and Inuit communities are sparser. According to the 2009–2010 Canadian Community Health Survey, age-standardized rates of self-reported diabetes among Métis were found to be 7.3 % compared to the non-Indigenous population which was 5 % (Fig. 13.1) [21]. In a recent report on a population-based study in Winnipeg, Manitoba, Métis aged 19 years and older were found to have age- and sex-adjusted diabetes rates that were higher (11.8 %) than compared to the provincial prevalence (8.8 %) [28]. An evaluation of diabetes in 14,480 Métis people in Ontario found the age- and sex-standardized prevalence to be 11.2 % compared to the general population which was 9 % [29].
According to the 2006 Aboriginal Peoples Survey, the crude rate of self-reported type 2 DM in Inuit was 4 % compared to the non-general population which was 5 % (Fig. 13.1) [30]. Although the prevalence of diabetes in the Inuit population has previously been documented to be lower than the other Indigenous groups, recent evidence highlights that it has markedly increased and is now comparable to the general Canadian population [1, 31].
In addition to higher overall prevalence and incidence rates compared to the general population, rates of gestational diabetes mellitus (GDM) are two- to fourfold higher in Indigenous women. The onset of type 2 DM in Indigenous people in Canada occurs at a much earlier age than in most other populations [25], and pediatric type 2 DM is a major public health concern [32, 33]. The increasing incidence of early age of onset of type 2 DM in Indigenous youth over the past several decades is concomitant with increases in the prevalence of childhood obesity [34–39]. Potential risk factors of childhood obesity in Indigenous school-aged children have included physical activity, fitness levels, TV watching, and dietary factors [36, 38, 39]. According to a recent published report from a national surveillance study, the Indigenous Canadian population has the highest incidence rate and is the largest single ethnic group that contributes to new-onset type 2 DM [40, 41]. The report highlights that 100/227 new diabetes cases belong to Indigenous peoples, and 11 % of these cases account for children younger than age 10 years [40, 41]. This accelerated onset of both obesity and type 2 DM suggests that the origins of these disorders may be traced back to infancy and/or the intrauterine environment [42, 43]. The early life/intrauterine risk of type 2 DM will be covered in more detail below.
Complications
Indigenous peoples in Canada experience a heavier burden of diabetes-related comorbidities compared to non-Indigenous peoples [44]. Indigenous peoples are burdened with a higher prevalence of microvascular complications, such as end-stage renal disease [44, 45], lower extremity amputations [46], and retinopathy [46–48] than their non-Indigenous counterparts with type 2 DM. Additionally, higher prevalence rates of macrovascular complications, including atherosclerosis [49] and cardiovascular disease [50], are also evident among Indigenous Canadians compared to non-Indigenous Canadians with type 2 DM [51].
Complications of diabetes in Indigenous peoples are exacerbated by limited social and economic resources, including inadequate access to health services due to geographical barriers [10, 52, 53]. Moreover, complications are likely more prominent in Indigenous populations as a result of an earlier age of diabetes onset. This population also has a higher prevalence of cardiometabolic and lifestyle risk factors for other chronic diseases, including smoking, obesity, and hypertension [25, 54].
One of the most remarkable and worrisome aspects of the type 2 DM complication profile in the Indigenous Canadian population relates to the very heavy burden of kidney disease. A study of incidence rates of diabetic end-stage renal disease in First Nations in Saskatchewan found that even when the higher prevalence of diabetes was taken into account, First Nations with diabetes were still seven times as likely as non-First Nations with diabetes to have end-stage renal disease [45]. Between 1980 and 2000, there was an eightfold increase in the number of Indigenous patients with diabetic end-stage renal disease [55, 56]. Indigenous dialysis patients with end-stage renal disease are found to have reduced rate of kidney transplantation [57]. The remote location of Indigenous patients on dialysis does not explain the lower rate of kidney transplantation among this group [58]. Although referral rates for kidney transplantation assessment are the same for Indigenous patients as for non-Indigenous patients, completion of transplantation documents and wait-listing for transplantation are delayed in Indigenous patients [59].
Indigenous Canadians with end-stage renal disease are more likely to reside in rural or remote locations compared to other dialysis patients. As a result, access to hemodialysis units may not be as readily available. Therefore, peritoneal dialysis might be very helpful for Indigenous patients requiring dialysis as it provides the ability to undergo dialysis at home without visiting a medical facility with a hemodialysis unit [60]. However, data from three Canadian provinces show that there are less frequent Indigenous users of peritoneal dialysis compared to non-Indigenous patients in Canada [60]. Also, patients who were on peritoneal dialysis were more likely to experience technique failure, compared to non-Indigenous patients; however, adjusted risk for death was similar to non-Indigenous patients [60].
Modifiable Risk Factors
Individual
Obesity and Body Composition
Among the modifiable risk factors for type 2 DM, overweight and obesity are the most well documented. The standard measure of body weight in population studies is body mass index (BMI). According to the 2004 Canadian Community Health Survey, the prevalence of obesity (defined using BMI) was higher among Indigenous Canadians (37.8 %) when compared to non-Indigenous Canadians (22.6 %) [61]. The prevalence of obesity was also higher among Indigenous children and youth (15.8 %), when compared to their non-Indigenous counterparts [61, 62].
When determining the prevalence of overweight and obesity in Indigenous peoples, it is salient to consider that the body dimensions of this group, and the Inuit population in particular, are different than other populations [63]. The Inuit are shorter in height and have shorter legs [63]. As a result, in order to improve the assessment of obesity in Inuit people, measures of body fat distribution, such as waist circumference, waist-to-height, and waist-to-hip ratio, should be employed [64–66]. In fact, a meta-analysis of over 300,000 individuals from different populations around the world found that waist-to-hip ratio was a better predictor than waist circumference and BMI for diabetes risk [66]. In a study on First Nations in Ontario, the 10-year cumulative incidence of diabetes was associated with high adiposity (defined as higher body mass index, percent body fat, waist circumference, or waist-to-height ratio) [27].
Smoking
Cigarette smoking has been associated with an increased risk of type 2 DM in a meta-analysis of 25 prospective cohort studies [67]. According to the meta-analysis, the risk of type 2 DM was greater for those who smoked >20 cigarettes a day than those who smoked <20 cigarettes a day [67]. Smoking prevalence is high in Indigenous populations and has been associated with complications of type 2 DM [44]. According to national data from the 2009–2010 Canadian Community Health Survey, the prevalence rates of self-reported smoking among Indigenous peoples aged 18 years and older were twofold higher than the rates of the non-Indigenous population [21]. Moreover, rates of daily tobacco smoking in Indigenous peoples were also 2.2–2.8 times higher than non-Indigenous people [21]. According to the 2012 Aboriginal People’s Survey, 52 % of Inuit aged 15 years and older smoked cigarettes daily, and another 9 % were occasional smokers [68].
In a study on First Nations in Ontario, former smoking was found to be associated with low beta-cell function, and current smoking was associated with high beta-cell function, independent of diabetes. Additionally, the association of smoking with insulin resistance varied depending on glycemic status [69]. In another First Nations population, smoking was found to increase incident diabetes risk in carriers of the HNF1A G319S allele. After stratification by baseline smoking status, HNF1A G319S carriers who were active smokers had increased risk of developing diabetes [70].
Diet
Research on the association of diet with type 2 DM has received considerable attention. Numerous dietary factors such as coffee, fiber, whole grains, and dairy products have been shown to have a protective effect on type 2 DM risk [71–74]. While some dietary factors including sugar-sweetened beverages and high consumption of fat have been associated with an increased risk for type 2 DM [75, 76]. Additionally, specific nutrients such as vitamin D have recently been investigated for their protective effects against the development of type 2 DM [77].
The nutritional habits of Indigenous peoples are of significant interest in the context of the management and prevention of type 2 DM [78]. Until relatively recently, Indigenous people of Canada were nomadic hunters and gatherers who had a traditional diet which consisted of large and small animals and birds (including the flesh and organs of moose, caribou, rabbit, ducks, geese, etc.), freshwater fish, marine fish and mammals, and some plant foods and, most notably, berries [79, 80]. In addition, the Iroquoian peoples of the Great Lakes and St. Lawrence River region farmed corn, beans, squash, and other crops. A significant body of research has documented a marked nutrition transition among Indigenous Canadians, in which the nutritional profile of Indigenous Canadians has changed from a traditional diet to a “market-foods” diet that is characterized by a higher intake in fat (especially saturated fat) and simple and high GI carbohydrates and low fiber [78, 81–84].
While the consumption of traditional foods has declined in general, Indigenous communities in some regions, most notably in the Northwest Territories and Yukon, have maintained a reasonably high degree of traditional food consumption [81, 85, 86]. Traditional food consumption is associated with beneficial impact on micronutrient intake. For instance, days with traditional food consumption are characterized by increased intakes of vitamins D, E, and B6, magnesium, and selenium. In addition, days when Indigenous participants consumed traditional food were characterized by higher intakes of energy as protein, whereas days when traditional food was not consumed were associated with a higher percentage of energy as carbohydrate, sucrose, and saturated and polyunsaturated fatty acids [81]. The potential benefits of high-fiber, high-fruit/vegetable/whole grain, low-fat, low-protein diets in the prevention of type DM among Indigenous Canadians have been studied [36, 38, 84, 87], and the findings have been largely consistent with those from other populations [88–90]. With regard to traditional foods, the consumption of seal oil and salmon has been found to be associated with a reduced risk of glucose intolerance in Indigenous people of Alaska [91]. In addition, in Cree from James Bay, higher traditional food consumption was associated with increased n-3 fatty acids [92]. Overall, however, very limited data are available regarding traditional food consumption and health outcomes among Indigenous peoples.
The transition to a market-foods diet has been accompanied by increasing prevalence of type 2 DM in Indigenous populations [10, 25]. A study in a First Nations community in Ontario found a high intake of total and saturated fat, and a diet high in GI foods was more common in people under 50 years of age, where rates of diabetes are showing their sharpest increase [83]. In another study in the same population, data was obtained using food frequency questionnaires to determine dietary patterns in the community. The intake of foods in the “junk foods” (chips/pop/candy/canned meat) category and fat (especially lard, consumed or used in preparation) category was associated with an increased risk of type 2 DM [84]. Similarly, a junk food dietary pattern (high-fat and high-sugar foods) identified in the Cree from Northern Quebec was associated with increased diabetes risk [92].
Another key public health nutrition problem affecting Indigenous communities is food insecurity. The prevalence of both individual and household food insecurity is much higher for Indigenous people compared to non-Indigenous people, with data from a national survey showing that 33 % of off-reserve Indigenous Canadians were food insecure compared to 9 % of non-Indigenous Canadians [93, 94]. After controlling for differences in household sociodemographic risk factors (including household income, highest level of education in household, household type, number of children, etc.), Indigenous households had two to six times greater odds for food insecurity compared to non-Indigenous households [93, 94]. In a recent national survey on Inuit, 41 % of Inuit aged 15 and older lived in households that experienced food insecurity [68].
Barriers to food security in Indigenous populations include income inadequacy and environmental pollution related to the impact of climate change on traditional food systems [86, 95]. A large number of Indigenous households rely on social assistance for income [93]. In fact, over 66 % of Indigenous households who received social assistance were food insecure [94]. In a study of access to traditional and market foods in 44 Indigenous communities across Arctic Canada, regional variation affected price and ability to purchase adequate food, with between 40 and 70 % of people saying they could afford enough food [96]. Additionally, Indigenous people reported inadequate access to fishing and hunting equipment, and 46 % of people could not afford to go hunting or fishing [96]. Changes in the local environment including changes in water levels have affected harvesting and traditional food acquirement in Indigenous communities [97]. Environmental contaminants in Indigenous traditional food resources such as heavy metals, radionuclides, and organochlorines put the health of Indigenous people at an increased risk [98]. In order to eradicate food insecurity among off-reserve Indigenous populations, government interventions must first address the great burden of poverty in this group by increasing income and social assistance funding for families [93, 95]. Overall, the considerable barriers to both traditional food and healthy market-food access discussed above have significant public health implications for both managing and preventing the type 2 DM epidemic currently being experienced by Indigenous communities in Canada.
Physical Activity
Engaging in physical activity has been well established to improve blood glucose control and has been identified as an important determinant in the prevention and management of type 2 DM [99–101]. A recent meta-analysis found that moderate intensity physical activity including brisk walking was negatively associated with the risk of type 2 DM [102].
Historically, Indigenous peoples engaged in activities such as hunting, fishing, and trapping to obtain sustenance [103]. However, as mentioned earlier, because of the nutrition transition, traditional activities are less prevalent, and this change has had a negative impact on the level of physical activity among Indigenous peoples and increasing the risk of type 2 DM and its complications [103]. According to a study in a First Nations community in Ontario, both physical activity and fitness were associated with lower insulin concentrations, suggesting that physical activity/fitness may be beneficial to the prevention of type 2 DM [104]. Television viewing was associated with childhood obesity in Mohawk children of Kahnawake [105]. Similarly, in First Nations people aged 10–19 years, 5 or more hours of television viewing/day was associated with a significantly higher risk of overweight than 2 or less hours of television viewing/day [36].
Intrauterine/Early Life Factors
High rates of youth-onset obesity and type 2 DM in Indigenous communities suggest that risk factors are operating very early in life, perhaps even in the intrauterine period. Recent research arising from the Developmental Origins of Health and Disease (DOHaD) paradigm has highlighted the importance to chronic disease etiology of a number of factors that have a significant importance in the context of type 2 DM in Indigenous Canadians [106], including high birth weight, gestational diabetes, and suboptimal breastfeeding.
High birth weight can have both immediate- and longer-term health consequences on infants, including shoulder dystocia, and an increased risk of type 2 DM [107, 108]. High birth weight appears to be closely associated with maternal diabetes and overweight. Consequently, as the prevalence of maternal obesity and gestational diabetes mellitus (GDM) continues to increase, higher birth weight babies will become increasingly prevalent as well [109].
There have been consistent observations of high birth weight in Indigenous Canadian babies [110, 111]. The prevalence of high birth weight in Cree was 34.3 % compared to 11 % in their non-Indigenous counterparts [112]. In a recent study on First Nations women in Northern and in Southern Quebec, First Nations women were more likely to have high birth weight babies than non-Indigenous women [113]. Similarly, a study reporting singleton births from Cree women living in rural or remote communities in Northern Quebec found prevalence rates of 2.4 % for low birth weight and 36.5 % for high birth weight. In the same study, infants who weighed >4500 g had a 14 % higher prevalence of birth injuries and were more likely born to women with GDM [114]. Another study on First Nations in Quebec reported a significant association between macrosomia and postnatal mortality [115].
Population Level
Environmental/Socioeconomic Risk Factors
Notwithstanding the importance of risk factors that occur at the level of the individual, it is increasingly being recognized that factors that characterize the local or broader social, environmental, and/or geographical environment are playing a critical role in the etiology of type 2 DM in Indigenous communities in Canada. These environmental risk factors for type 2 DM have emerged largely from historic policies of colonization unique to the Indigenous context [116]. In particular, the health and social conditions of Indigenous peoples vary significantly depending on residence on-reserve versus off-reserve and in rural versus urban areas [117]. Living in remote or rural areas may lead to limited opportunities for education and employment and reduced access to a safe and healthy food supply [20, 117]. Geographic and language barriers may also result in reduced access to health-care services [118]. As well, there is limited availability of culturally appropriate services in Indigenous communities [20, 119]. These limitations may potentially affect the prevalence and distribution of type 2 DM in Indigenous peoples by affecting the level of care and treatment available for type 2 DM and its complications [117].
Non-modifiable Risk Factors
Genetics
Genome-wide association studies (GWAS) of type 2 DM over the past several years have identified numerous susceptibility genes for type 2 DM [120–123]. Specific population groups have been shown to possess predisposing alleles to type 2 DM [124]. Indeed, high rates of type 2 DM in Indigenous communities in Canada suggest an inherited component. Early interest in the search for a single “Thrifty” gene [125] explaining the high type 2 DM burden in Indigenous Canadians was unsuccessful, due to the fact that type 2 DM in these communities is very likely caused by the cumulative small effects of multiple genes operating on the background of a detrimental environment [10, 126]. Nonetheless, a private mutation in the HNF1α gene (namely, G319S), restricted to the Oji-Cree population of Northwestern Ontario and Northeastern Manitoba, has been shown to be associated with an increased risk for type 2 DM [127]. In fact, by 50 years of age, HNF1α S319 has specificity (97 %) and positive predictive values (95 %) for the development of diabetes in the Oji-Cree population [106].
Clinical Care
For Indigenous people, health-care access and delivery depends on location, with urban and off-reserve Indigenous peoples accessing health care from provincially funded services. In contrast, as a part of the set of obligations arising from signed treaties with the federal government, health-care delivery on-reserves is delivered by federally operated nursing stations and health centers. The First Nations and Inuit Health Branch (FNIHB) provides health benefits to First Nations and Inuit that are noninsured by provincial insurance plans, including prescription drugs and dental and vision coverage [128, 129]. Physician services and hospital care are provided by the government of each province or territory [128]. The federal government’s role in Indigenous health occurs primarily through public health and intervention strategies [128]. With regard to federal programs that specifically target diabetes, the Aboriginal Diabetes Initiative supports health promotion and type 2 DM prevention programs which are disseminated by community diabetes workers [129].
The current health-care delivery system in Indigenous communities consists predominately of acute and intermittent care management instead of coordinated chronic disease care [130]. As a result of geographical isolation, limited staff and other nonphysician health professionals provide clinical care in these communities [118]. Additionally, hospital admissions for ambulatory care conditions are much higher in Indigenous communities [131–133], and there is poor communication between provincially funded hospitals and federal nursing care centers in most Indigenous communities [33].
Research has documented suboptimal clinical care for diabetes among on-reserve First Nations peoples in Canada. These clinical care gaps are attributable to geographical isolation, limited health-care staff, poor chronic disease management, limited surveillance, and high staff turnover [134]. Despite the high burden of chronic disease in the Indigenous population, including type 2 DM, the use of primary health care is lower among Indigenous populations compared to the general population [132].
National data from the Western provinces (British Columbia, Alberta, Saskatchewan, and Manitoba) on type 2 DM burden and clinical care gaps found that the age-standardized hospital discharge rate was seven times higher in First Nations peoples living on- and off-reserve compared to the general population [119].
There is a higher mortality rate (19.5 per 100,000) due to type 2 DM in Indigenous Canadians compared to non-Indigenous Canadians (13.3 per 100,000) [135]. Although there is less frequent use of primary health services among Indigenous peoples in Northern or isolated communities [136], the per capita health-care costs of Indigenous populations with and without type 2 DM are much higher compared to non-Indigenous populations [137]. Particularly, health-care usage, including physician appointments, hospital visits, and dialysis, is 40–60 % higher among First Nations in Saskatchewan with type 2 DM compared to the non-Indigenous population without type 2 DM [137].
Recently, a new program called the Transformation of Indigenous Primary Healthcare Delivery (FORGE AHEAD) has been initiated in five First Nations communities across Canada to improve diabetes management through the development of community-based, culturally relevant primary health-care models. FORGE AHEAD also aims to develop appropriate access to services in First Nations communities [138].
Primary Prevention
There is a great necessity for Indigenous-specific diabetes prevention and intervention strategies that consider the unique cultures and traditions of First Nations, Métis, and Inuit people. Interventions which include tenets such as community involvement, face-to-face interventions, development of skills to promote behavior change, and the dissemination of educational and nutritional knowledge are required to alleviate the burden of type 2 DM in marginalized communities [139].
In the late 1990s, the government of Canada established the Aboriginal Diabetes Initiative to help improve the heavy burden of type 2 DM among First Nations, Inuit, and Métis [129]. The program has been delivered in three phases. The first phase, ADI Phase 1 (1999), allocated $115 M over 5 years for health promotion and primary prevention programming. The second phase, ADI Phase 2 (2005–2010), allocated $190 M over 5 years to strengthen community-based health promotion and diabetes prevention activities. The current phase, ADI Phase 3 (2010–2015), has allocated $275 M for continued support of health promotion and diabetes prevention activities and services.
Related posts:
 The Global Burden of Diabetes: An Overview
The Global Burden of Diabetes: An Overview
 Diabetes in Indigenous Australians and Other Underserved Communities in Australia
Diabetes in Ethnic Minorities and Immigrant Populations in Western Europe
Diabetes in Indigenous Australians and Other Underserved Communities in Australia
Diabetes in Ethnic Minorities and Immigrant Populations in Western Europe
 Type 2 Diabetes in the Middle East and North Africa (MENA)
Type 2 Diabetes in the Middle East and North Africa (MENA)
 Primary Prevention of Type 2 Diabetes: An Imperative for Developing Countries
Primary Prevention of Type 2 Diabetes: An Imperative for Developing Countries
 Diabetes in China and the Western Pacific Region
Diabetes in China and the Western Pacific Region
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


