Melanoma arises from the malignant transformation of the melanocyte, the cell responsible for the production of the pigment melanin. Precursor melanocytes arise in the neural crest and, as the fetus develops, migrate to multiple areas in the body including the skin, meninges, mucous membranes, upper esophagus, and eyes. Melanomas can arise from any of these locations through the malignant transformation of the resident melanocytes. By far the most common location is the hair follicle-bearing skin arising from melanocytes at the dermal/epidermal junction. In the National Cancer Database, 91.2% of melanomas are cutaneous, 5.3% are ocular, 1.3% are mucosal, and 2.2% are of unknown primary site.1 Each of these types has significant differences in the etiology and genetic makeup, in particular related to the degree of ultraviolet (UV) radiation exposure and their frequency of driver oncogenic mutations. The current understanding of melanoma biology comes from studies of genetic analyses of melanomas correlated with clinicopathologic presentations, which have elucidated two key features of this cancer: (1) cutaneous melanoma, as opposed to mucosal or uveal melanoma, is usually a carcinogen-induced cancer with a high mutational load, demonstrated by the molecular fingerprinting of UV light damage, and (2) the majority of melanomas are dependent on a particular oncogenic signaling pathway, the mitogen-activated protein kinase (MAPK) pathway, through usually mutually exclusive driver mutations in cKit, NRAS, BRAF, GNAQ or GNA11.2,3,4,5,6 Cutaneous melanomas arising from the trunk and extremities, which are associated with intermittent UV radiation exposure, have high rates of BRAF (50%) or NRAS (20%) mutations.2,7,8 Mucosal and acrolentigenous melanomas, with low rates of UV radiation exposure, have lower rates of BRAF mutations (5% to 20%) and higher rates of KIT mutations (5% to 10%).2 The great majority of uveal melanomas have mutually exclusive mutations in the alpha subunits of G-protein-coupled receptors GNAQ and GNA11.3,4
The primary focus of this chapter is on cutaneous melanoma, but summary information is presented for the other forms of melanoma, as well as on the subtypes of cutaneous melanoma.
MOLECULAR BIOLOGY OF MELANOMA
Mutational Landscape in Melanoma
Studies of whole exome sequencing (sequencing of the approximately 1.6% of the genome that encodes for expressed proteins) and whole genome sequencing of melanomas compared to matched normal DNA of the same patients are leading to a greatly improved understanding of the genomic alterations in melanoma. The studies of the mutational load of cutaneous melanomas by next generation sequencing demonstrate that melanoma has significantly more sequence variations per megabase of DNA compared to most other cancers. For example, melanomas have 15 times more mutations per megabase of DNA than colorectal cancer and 4 times more than lung cancer.9 As a high proportion of these mutations are cytosine to thymine (C>T) substitutions, typical of UV radiation-induced thymine dimmers, it is highly likely that the high rate of sequence variants in melanoma is due to the role of UV as the principal carcinogen in the disease.10,11,12
Two studies have reported on exome sequencing of relative large series of melanomas compared to normal matched DNA. After sequencing the exomes of 147 melanomas, it became evident that sun-exposed melanomas had markedly more UV-like C>T somatic mutations compared to sun-shielded acral, mucosal, and uveal melanomas. These studies confirmed the recurrent mutations in BRAF, NRAS, and cKit. Newly identified recurrently mutated cancer genes included PPP6C, encoding a serine/threonine phosphatase in 12% of sun-exposed melanomas, and were mutually exclusively in tumors with mutations in BRAF or NRAS. Furthermore, an activating mutation in RAC1(P29S) was noted in 9.2% of sun-exposed melanomas.11 In a similar study, analysis of large-scale melanoma exomes from 121 paired samples12 also confirmed the recurrent BRAF, NRAS, and cKIT mutations, and discovered six recurrently mutated melanoma genes (PPP6C, RAC1, SNX31, TACC1, STK19, and ARID2), two of which are the same as in the other study. Integration with chromosomal copy number data contextualized the landscape of driver mutations, providing oncogenic insights in BRAF- and NRAS-driven melanoma as well as those without known NRAS/BRAF mutations. In this study, the authors found a higher than expected number of genetic events dysregulating the RB and p53 pathways, which had previously thought to be mostly intact in melanoma.12
The first fully sequenced whole genome of any cancer was a melanoma cell line compared to a lymphoblastoid cell line generated from the same patient to provide the comparing source of normal DNA.10 This study provided the first comprehensive catalogue of somatic mutations from an individual cancer. The dominant mutational signature reflects DNA damage due to UV light exposure. It also revealed an uneven distribution of mutations across the genome, with a lower prevalence in gene footprints, which indicated that DNA repair preferentially functioned in areas with transcribed regions. There are ongoing efforts to perform whole exome sequencing in large panels of melanomas. The largest effort is The Cancer Genome Atlas. It will report on whole exome sequencing in over 500 melanoma samples compared to normal exomes, with a subset of cases additionally undergoing whole genome sequencing, DNA methylation studies, RNA sequencing, microRNA sequencing, and reverse phase protein array analysis of phosphorylated proteins.
The studies of whole genome sequencing will be important to understand melanoma genetic alterations in nontranscribed genes since there can also be recurrent mutations in them. This is exemplified by the demonstration of two very common mutations in the promoter of telomerase reverse transcriptase (TERT) by two independent research groups. TERT is the gene coding for the catalytic subunit of telomerase. In one of the studies,13 mutations in the TERT promoter were reported in 71% of melanomas examined. The mutations increased the transcriptional activity from the TERT promoter by two- to four-fold. This information may be of high relevance beyond melanoma, since examination of 150 cancer cell lines derived from diverse tumor types revealed the same mutations in 24 cases (16%). The other group reached the same conclusion by investigated a melanoma-prone family through linkage analysis and high-throughput sequencing.14 They identified the same TERT promoter mutations as disease-segregating germline mutations. When they screened TERT promoter mutations in sporadic melanoma, they found them in 74% of human cell lines derived from metastatic melanomas and in 33% of primary melanomas.
Driver Mutations in Melanoma
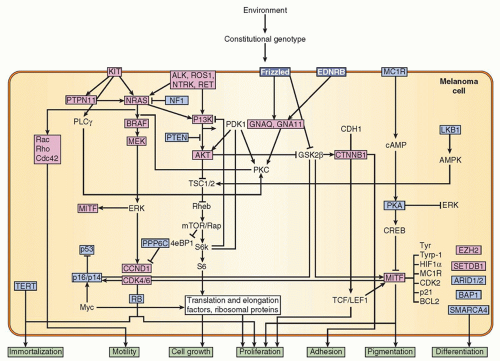
Melanoma has become a notable example of a cancer histology dependent upon driver oncogenic mutations in the MAPK pathway, with additional genetic alterations in other pathways leading to uncontrolled cell growth and avoidance of apoptosis (Fig. 38.1). There is evidence of MAPK activation by defined point mutations in at least 70% of melanomas, resulting in constitutive signaling leading to oncogenic cell proliferation and escape from apoptosis.15 The aberrations that lead to MAPK pathway activation in most cutaneous and mucosal melanomas consist in usually mutually exclusive activating mutations in the receptor tyrosine kinase KIT (2% to 3%), the G-protein neuroblastoma RAS viral oncogene homolog (NRAS) (15% to 20%), and the serine-threonine kinase BRAF (40% to 50%).3,4,5,6 Uveal melanomas have a distinct set of driver mutations in GNAQ and GNA11, which are the alpha subunits of G-protein-coupled receptors.3,4
Mutations in KIT are found in exons 9, 11, 13, and 17, and there is no one predominant point mutation.6 Because of this, molecular testing for KIT mutations must evaluate multiple regions of the gene by extended sequencing or multiplexed polymerase chain reaction (PCR) tests. Emerging evidence suggests that not all KIT mutations activate its function, resulting in some mutations being insensitive to KIT inhibitors used for patient treatment.16 NRAS mutations cluster in the RAS hotspot mutation site Q61, usually Q61L and less frequently Q61R and Q61H. NRAS mutations are more frequent in older individuals and are equally common in melanomas arising from the skin with chronic or intermittent sun damage.2,17 The vast majority of BRAF mutations in melanoma involve a substitution for valine at the 600th amino acid position to glutamine (V600E).5,18 The frequency of the BRAF V600E mutation is inversely correlated with age since it is most frequent in melanomas that appear on the skin without chronic sun damage in young adults. BRAF V600K is the second most common variant, which increases in incidence with age. V600D or V600R mutations are much less frequent.8 Overall, up to 90 different point mutations have been described in BRAF in different cancers, some of which are activating and others are inhibiting its enzymatic activity.18
Figure 38.1 Signaling pathways disrupted by genetic alterations and their relationship to the hallmarks of melanoma. Proteins boxed in red are affected by gain-of-function mutations; those boxed in blue are affected by loss-of-function mutations. (Source: Bastian BC. The molecular pathology of melanoma: an integrated taxonomy of melanocytic neoplasia. Ann Rev Pathol Mech Dis 2014;9:239-271.)
Aberrations in the phosphoinositide 3-kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin pathway, including the phosphatase and tensin homolog (PTEN), are also noted in a significant number of melanomas, but these do not seem to function as true drivers of the malignant phenotype. PTEN alterations include missense mutations, deletions, and insertions, as well as loss of heterozygosity and epigenetic silencing, making interrogation for mutations and genomic rearrangements in PTEN necessary.19,20 The pathogenesis of melanoma, like most other cancers, requires the presence of a driver oncogene and the dysregulation of cell cycle control and apoptosis to provide the full oncogenic signaling and ability to grow autonomously. These happen with the frequent mutations or genetic deletions of CDKN2A, cyclin D1, or the amplification cyclin-dependent kinase 4.21
Progression of Melanocytes to Cutaneous Melanoma
Genetic Events in Melanocyte to Melanoma Progression and Oncogene-Induced Senescence
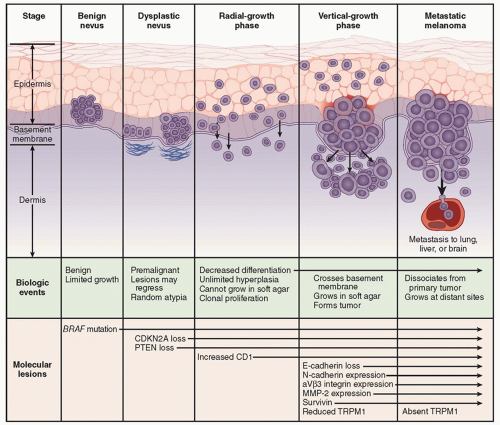
BRAF and NRAS are founding mutations of cutaneous melanoma that are frequently present in benign nevi.22 Despite of the presence BRAF and NRAS mutations, nevi have an exceedingly low proliferative activity and infrequently progress to melanoma. This is explained because of the phenomenon of oncogeneinduced senescence preventing malignant progression to melanoma, where these mutations require functioning with additional genetic events that lead to dysregulation of cell cycle control to result in the development of a progressive melanoma.15,23 The model for oncogene-induced senescence in melanoma is based on the identity of the main driver mutations (BRAF and RAS) in nevi, the initial phase of proliferative activity they spark, the formation of a benign nevus in association with the induction of senescence markers (cell cycle arrest, induction of the tumor suppressor p16INK4a, endoplastic reticulum stress markers and increased SA-βGal activity, and possibly additional senescence biomarkers), and the subsequent cessation of expansion, which is typically maintained for decades.24
Figure 38.2 Biologic events and molecular changes in the progression of melanoma. (From Miller AJ, Mihm MC Jr. Melanoma. N Engl J Med 2006;355:51-65.)
Cellular Changes in Melanocyte to Melanoma Progression
The transition from melanocyte to metastatic melanoma involves several histologic intermediates, including melanocytic atypia, atypical melanocytic hyperplasia, radial growth phase melanoma, vertical growth phase melanoma, and metastatic melanoma. Atypical melanocytes arising in a preexisting nevus or de novo are very common but rarely progress to melanoma. However, some patients develop confluent atypical melanocytic hyperplasia at the dermal/epidermal junction or nests of atypical melanocytes in the epidermis or at the dermal/epidermal junction. As this process progresses, it reaches a point at which a diagnosis of melanoma is warranted.
Early cutaneous melanomas usually proceed to grow radially, and this is called the radial growth phase (RGP) of melanoma, which may continue for years before progressing to the vertical growth phase (VGP) (Figs. 38.2 and 38.3). The RGP of a cutaneous melanoma may include either melanoma in situ or superficial invasion into the papillary dermis, or both. Melanomas in RGP present clinically as enlarging macules or very minimally raised papular lesions, which are typically (but not always) pigmented. These lesions are rarely symptomatic. If not recognized, these lesions typically progress to the VGP, manifest clinically by a nodular growth of the lesion, often described by the patient as a lesion that began to “raise up.” This vertical growth usually arises as a nodule within the RGP component and encompassing only part of the RGP (see Fig. 38.3A,C). Thus, the VGP appears to represent further steps in the process of malignant transformation due to clonal changes in the cells of the RGP.
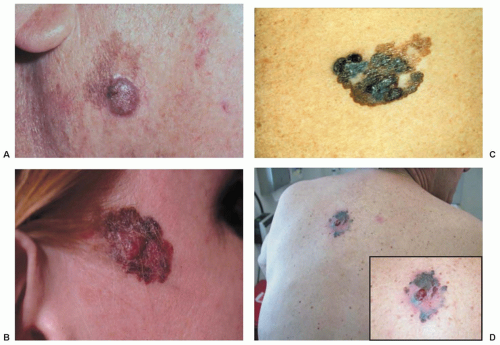
Figure 38.3 (A) A nodule of vertical growth phase melanoma arising from a radial growth phase pigmented macule on the right cheek. (B) Superficial spreading melanoma, 2.9 mm thick, arising on the temple of a young woman. There were microscopic satellites, and the patient died of disease within several years. (C) Superficial spreading melanoma with all the classic features of the ABCD mnemonic (asymmetry, border irregularity, color variation, and diameter >6 mm). (D) Large, ulcerated 2.5 mm superficial spreading melanoma with regression in elderly man.
Some melanomas present as metastatic melanoma in lymph nodes, skin, subcutaneous tissue, or visceral sites without an apparent primary cutaneous site. In some cases, these have been associated with a history of a regressed primary melanocytic lesion. In other cases, such an explanation is less clear. In all of these cases, the prospect of early diagnosis of melanoma is compromised, and the risk of melanoma-associated mortality is increased.
EPIDEMIOLOGY
Malignant melanoma is the sixth most common US cancer diagnosis. The actual incidence of melanoma is increasing more rapidly than that of any other malignancy. It was estimated that 76,690 men and women (45,060 men and 31,630 women) will be diagnosed with and 9,480 men and women will die of melanoma of the skin in 2013.25 This amounts to 4% of new cancer diagnoses and 1.5% of cancer deaths. In the early part of the 20th century, the lifetime risk of a white person developing melanoma was approximately 1 in 1,500. Currently, 1 in 49 men and women will be diagnosed with melanoma of the skin during their lifetime. Its incidence is second only to breast cancer for women from birth to age 39 years; similarly, it is the second most common cancer diagnosis for men through age 39 years, slightly less common than leukemia.26 Overall 5-year survival rates for melanoma have increased from 82% in the late 1970s (1975 to 1977) to 91% in the more recent era (2002 to 2006).26
This is a disease that disproportionately affects whites over African Americans, Asians, or Hispanics. In the United States, whites account for 98.2% of cutaneous melanomas reported in the National Cancer Database, with African Americans accounting for 0.7% and Hispanics accounting for 1.1%.1 This is best explained by a combined effect of UV sunlight exposure and fair skin. It is most striking that the highest per capita incidence of melanoma worldwide is in Australia, and that this high incidence afflicts primarily the Australians of Western European descent who have fair skin, and not the darker-skinned aboriginal population. It is also notable that these fair-skinned European descendants who moved to Australia have much higher incidences of melanoma than the Western European populations that remain in the higher latitudes of Europe. In migrant populations, individuals who move during childhood to areas with greater sun exposure develop melanoma at rates higher than those of their country of origin and similar to those of their adopted country.27
In nonwhite populations, there is a much higher proportion of melanomas in acral (subungual, palmar, plantar) and mucosal locations. However, the incidences of those types of melanoma are similar across races. Their higher relative proportion in Asians and African Americans can be best explained by the disproportionate increase in nonacral cutaneous melanomas in fair-skinned whites rather than by an absolute increase in risk of acral and mucosal melanomas in nonwhite populations.
Ocular and nonacral cutaneous melanomas are 50- to 200-fold more likely in white populations than in nonwhite populations, but melanomas in acral and mucosal sites are within twofold of each other across racial groups. Similarly, the increased incidence of melanoma over the last few decades can be explained primarily by increased incidence in white populations, not in nonwhite populations.28 These observations support the hypothesis that most cutaneous melanomas in white populations are etiologically related to sun exposure but that there may be a baseline risk of melanoma in other locations that is unrelated to sun damage. There are significant molecular differences between acral melanomas and melanomas arising on the skin associated with chronic sun damage, with B-RAF and N-RAS mutations in approximately 80% of melanomas on chronically sun-damaged skin, whereas those mutations were uncommon in melanomas from acral or mucosal sites or from skin without chronic sun damage.2
CHANGES IN INCIDENCE
Data from the Surveillance, Epidemiology, and End Results program reveal an increase in age-adjusted melanoma incidence rates from 8.2 per 100,000 in the 1970s (1974 to 1978) to 18.7 per 100,000 in more recent years (1999 to 2003).29 From 1990 to 2003, during which there was a 16% decrease in male cancer deaths overall for all cancers, there was a 2% increase in mortality rate from melanoma. From 1991 to 2003, during which there was an 8% decrease in cancer deaths overall for women, there was only a 4% decrease in mortality rate associated with melanoma.26
In Australia, and to a lesser extent in the United States, there has been a substantial increase in awareness about melanoma and the value of screening by total-body skin examinations. There also has been a greater proportion of patients diagnosed at earlier and noninvasive stages of disease. Thus, part of the increase in incidence may be explained by increased early diagnosis of lesions with low metastatic potential. However, there has also been a significant increase in mortality from melanoma over the last few decades.29
GENDER AND AGE DISTRIBUTION
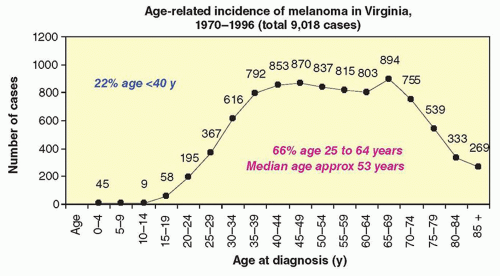
In the United States and Australia, the gender ratio of melanoma at diagnosis is 2 male to 1 female, but it depends on the age group. Analysis of incidence data for invasive melanoma diagnosed from 1992 to 2006 from 12 cancer registries that participate in the Surveillance, Epidemiology, and End Results program of the National Cancer Institute revealed that, by age, the men-to-women rate ratio ranged from 1.3 (95% confidence interval [CI], 1.2 to 1.3) for ages 40 to 64 years for incidence to 2.6 (2.5 to 2.7) for older than 65 years for both incidence and mortality. However, between the age of 15 and 39 years old, melanoma is more common in females (rate ratio = 0.6).25 The median age of melanoma patients has increased from 51 years in the 1970s (1974 to 1978) to 57 years in a more recent time period (1999 to 2003). Nonetheless, the median age for diagnosis of melanoma is approximately 10 years lower than the current median age of diagnosis for the more common solid tumors, such as colon, lung, or prostate cancer. The large majority (approximately 80%) of patients with melanoma are diagnosed in the productive years from age 25 to 65 as shown for a representative population from the state of Virginia (Fig. 38.4). Melanoma is common in patients in their 20s and older, but it also is observed in teenagers, and occasionally even in infants and neonates. For women aged 25 to 35 years, melanoma is the leading cause of cancer-related death.
Figure 38.4 Age-related incidence of melanoma in Virginia, 1970 to 1996 (total of 9,018 cases).
MELANOMA IN CHILDREN, INFANTS, AND NEONATES
Diagnosis and management of melanoma in children, infants, and neonates is complicated by several factors: (1) excisional biopsy of skin lesions often is not feasible under local anesthesia in young children, and (2) pigmented skin lesions with substantial cellular atypia but with structural symmetry may be Spitz nevi, which typically have benign behavior. Thus, some young patients with changing pigmented skin lesions are observed longer than would be advisable because biopsy is more problematic than in most adults. In addition, young patients may undergo incomplete shave biopsy to avoid a full-thickness excision, and information is lost about the architecture of the lesion, leaving a diagnostic dilemma between melanoma and Spitz nevus. Even in the best of circumstances, some melanocytic tumors are difficult to diagnose with certainty. This has led to a formal definition of melanocytic tumors of uncertain malignant potential.30
Melanoma deaths in children and young adults have a large effect on total years of life lost because of melanoma. Current recommendations for management of melanoma in children and infants are the same as for adults, and outcomes are generally believed to be comparable.31
ANATOMIC DISTRIBUTION
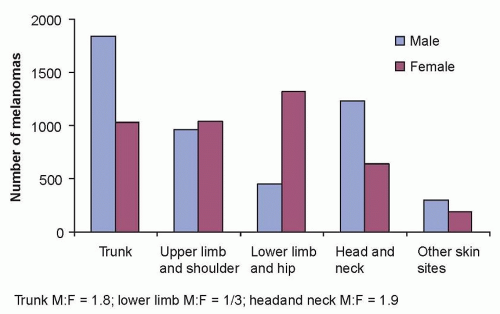
Cutaneous melanoma can occur at any skin site in the body. The most common sites in males are on the back and in the head and neck regions. In women, the most common sites are in the lower extremities, commonly below the knee (Fig. 38.5). Lentigo maligna melanoma (LMM) most commonly arises on sun-damaged surfaces of the head and neck in older patients. Acral lentiginous melanoma (ALM) is most common on subungual and other acral locations.
Figure 38.5 Incidence of melanoma in Virginia, 1970 to 1996, by gender.
ETIOLOGY AND RISK FACTORS
Ultraviolet Light Exposure
The demographic features of cutaneous melanoma have implicated UV light exposure as a major etiologic factor in the development of melanoma. Multiple studies continue to support an etiologic association between UV irradiation and melanoma.32 UVC radiation is generally absorbed by the ozone layer. UVB radiation (290 to 320 nm) is associated with sunburn and induction of tanning by melanin pigment production. There are substantial data to support its etiologic role in melanoma.32 There is also some evidence implicating UVA radiation (320 to 400 nm), although UVA is more associated with chronic sun damage changes.33 However, the relative role of each type of UV irradiation in melanoma etiology is debated. Animal data suggests that sun exposure early in life increases the risk of melanoma. Human skin grafted on mice will develop nevi and melanomas in the presence of UVB irradiation, further supporting the role of UVB irradiation in melanoma.34 Similar to the animal modeling, sunburns early in life have been implicated in melanoma incidence.35 However, chronic sun exposure in individuals who tan well may even be protected against melanoma. The role of sunlight intensity and frequency is debated, but both chronic and intermittent exposure may be relevant.32 Current data suggest that UV radiation causes melanoma by a combination of DNA damage, inflammation, and immune suppression.36
Tanning bed use has been implicated in the etiology of melanoma, in particular tanning bed use in adolescence or early adulthood.37 Tanning bed use has been formally classified as a carcinogen, and increased awareness of the harmful effects of UV exposure promise to control the increase in melanoma incidence.
Physical Traits
Several physical traits have been linked to increased incidence of cutaneous melanoma. These include blond or red hair, green or blue eyes, presence of multiple (>100) melanocytic nevi, and five or more atypical nevi. A prior diagnosis of melanoma is associated with an eight-fold increased risk of developing a secondary melanoma.
Familial Predisposition
It has been estimated that 5% of melanomas occur in high-risk families with an autosomal dominant inheritance with incomplete penetrance.38 The most frequent and highest penetrance melanoma susceptibility gene is a germline mutation in CD-KN2A, a tumor suppressor gene that encodes for two different proteins, p16INK4A and p14 ARF.39 These proteins control cell cycle progression and apoptosis, and have roles in correcting DNA damage and cellular senescence. CDKN2A mutations have been reported in approximately 25% of melanoma-prone families, but this frequency varies highly on the selection criteria used and the region of the world where it is studied. The rare autosomal dominant inherited familial atypical multiple mole melanoma-pancreatic cancer syndrome is associated with CDKN2A mutations, and less frequently to BRCA2 mutations.40 Another germline mutation linked to familial melanoma is cyclin-dependent kinase 4, which is linked to the function and p16INK4A and controls the retinoblastoma pathway. A germline mutation in microphthalmia-associated transcription factor (MITF E318K) represents a medium-penetrance susceptibility gene predisposing to familial melanoma, as well as to sporadic melanoma and renal cell carcinoma.41,42 The E318K mutation in MITF disrupts sumoylation and enhances transcription of MITF-responsive genes. Other common risk factors include dysplastic nevus syndrome, xeroderma pigmentosum, and a family history of melanoma even without the known genetic traits. The association of melanoma with Li-Fraumeni syndrome, with germline mutations in p53, is currently unclear.43
Pregnancy and Estrogen Use
Older literature suggested anecdotally that the incidence of melanoma was higher in pregnant females and that they had a particularly bad outcome. However, multiple systematic and larger studies have shown no evidence of any negative (or positive) impact of prior, concurrent, or subsequent pregnancy on clinical outcome.44,45 Similarly, there is no clear prognostic relevance for birth control pills or estrogen replacement therapy.46 The prior sense of an apparent association of pregnancy and melanoma may be due to melanoma being the second most frequent cancer in females of childbearing age. The general recommendation for treatment of women with melanoma diagnosed during pregnancy is to manage them in the same fashion as patients who are not pregnant. Depending on the time during pregnancy at which a melanoma is diagnosed, there can be circumstances in which radiologic imaging may be limited because of concern for the fetus, and major surgery may be delayed until the fetus is at an age when it can survive independently. However, the excision of a primary melanoma certainly can be done in almost any circumstance, under local anesthesia.
The other related question often asked by patients is whether it is advisable to become pregnant and to bear a child after treatment for melanoma. As just stated, there is no evidence that a subsequent pregnancy adversely impacts outcome. However, the more interesting and challenging question is the more personal or social issue of the potential for premature parental death due to melanoma. Thus, it is helpful for patients to understand their risk of future recurrence and melanoma-related mortality because that translates into the risk that the child will grow up losing a parent. Measures of the risk of future disease progression can be defined based on the initial prognosis and the subsequent elapsed time without recurrence, and such information may help to guide patients with this challenging question.47
PREVENTION AND SCREENING
Melanomas diagnosed and treated during the RGP have an excellent prognosis. Thus, prevention and early diagnosis can have a great impact on decreasing melanoma morbidity and mortality. The apparent leveling off of melanoma-related mortality rates in Australia and the United States likely is the result of better screening and prevention.
Sun Protection
UV exposure and sunburns, in particular, appear to be etiologic in most melanomas. Thus, protection from UV light, especially in fair-skinned individuals, is believed to have substantial benefit in preventing melanoma.
A clinical trial has provided evidence that regular sunscreen use helps prevent melanoma.48 This was a randomized trial from March 1992 to August 1996 of 1,621 randomly selected adult residents of a Queensland township in Australia with an initial primary end point testing the prevention of squamous cell and basal cell carcinomas, which the study did demonstrate.49 Prevention of the development of melanoma was a prespecified secondary end point. Participants were randomly assigned to either a planned sunscreen intervention group or a control group using sunscreen at their discretion. The intervention group received broad-spectrum, sun protection factor (SPF) 16 sunscreen every morning, and was instructed to reapply the sunscreen after a long sun exposure, heavy sweating, or after bathing. After a 10-year follow-up, regular sunscreen use decreased by half the rate of developing new melanomas. This conclusion was based on 11 participants in the intervention group and 22 in the control group being newly diagnosed with either invasive or in situ melanoma (p = 0.051). The incidence of invasive melanoma decreased by 73% in the intervention group compared with the control group (3 versus 11 patients, respectively; p = 0.045). Therefore, this study provides evidence that use of sunscreen can decrease the incidence of melanoma development.
There are limitations inherent in sunscreen use as the primary means to protecting from UV light damage. One is that certain body sites are not easily covered with sunscreen, such as the scalp. More important, even “waterproof” sunscreens wash off or become less effective with time. Most people also forget to reapply sunscreens frequently enough and may still get burns. There are also sociologic issues, which may differ for different populations and are arguable. However, it is worth considering the provocative findings of a study performed on young adults from Western Europe, who were randomized to receive either SPF10 or SPF30 sunscreen. In a blinded fashion, they were asked to report sun exposure times and sunburns. The number of sunburns was the same in both groups, and sun exposure was greater in the SPF30 group, suggesting that some populations may stay in the sun until they get a burn, and that sunscreen simply helps them to stay in the sun longer.50 The sun-seeking behavior has been related to an evolutionary need that favored UV exposure to make vitamin D in the skin in populations that migrated to areas of the world with lower sun exposure. In mouse models, the exposure to UV light was linked to increased production of beta-endorphins and recurrent seeking of UV exposure.51
It is safe to say that the best protection from the sun is a building, the next best is protective clothing, and the third best is sunscreen. Patients should be advised to use all three. Avoiding midday sun from about 11 a.m. to 3 p.m. by staying indoors is advised, as well as wearing clothing with a thick enough weave that it blocks sunlight, or a formal SPF rating, when possible. Hats are particularly helpful for the face and scalp, which often are highly exposed to sunlight and not so readily covered fully with sunscreen. Otherwise, sunscreen can provide protection to sunexposed areas when outside.
Screening for Early Diagnosis
Self-Examination
For many patients, they, their spouses, or other family members may be able to screen effectively for new suspicious skin lesions, and this should be encouraged. It is more common for women to detect melanomas than for men to do so, either for themselves or for their partners. In any case, there is value in educating patients about how to detect melanomas if they are at high risk. As many as half of melanomas are identified by the patient or family,52 and patient self-examination has been associated with diagnosis of thinner melanomas.53 Teaching aids for patients on how to perform skin self-examination are available from the American Cancer Society and the American Academy of Dermatology. Patients with melanoma or at high risk should be seen regularly by a dermatologist. It is reasonable to suggest that patients perform skin selfexaminations more often than their dermatology visits, although there are no proven guidelines. Doing a self-examination once a month may be the easiest for the patient to remember.
The role of skin cancer screening to decrease incidence and mortality from cutaneous melanoma has been prospectively studied in the Schleswig-Holstein project.54 This was an observational study comparing trends in melanoma mortality in a population-based skin cancer screening project conducted in the northern German region of Schleswig-Holstein, compared to neighboring regions in Germany and Denmark where no such screening was conducted. From July 1, 2003, to June 30, 2004, 360,288 individuals aged 20 years were screened by whole-body examination. They reported that mortality in Schleswig-Holstein melanoma declined by 48% when analyzed using log-linear regression to assess mortality trends. No such change in melanoma mortality rates was noted in the studied adjacent regions. This study provides strong evidence that skin cancer screening programs may reduce melanoma mortality.54
Management of the Patient with Numerous Atypical Moles
Some patients have numerous atypical moles. This presentation is commonly described as atypical mole syndrome, dysplastic nevus syndrome, or B-K mole syndrome.55 These patients have a heightened risk of melanoma, and this is commonly a familial feature. When associated with a family history of melanoma, patients with dysplastic nevus syndrome have a risk of melanoma that may approach 100%. These patients deserve particular attention to melanoma prevention through sun protection and to early diagnosis through aggressive screening. However, the optimal approach for screening is not defined. At a minimum, routine skin examinations by a dermatologist are usually recommended, as often as every 3 months. Visual inspection of the atypical nevi may be augmented by routine digital photography to facilitate detection of subtle changes in radial growth or other changes over time. Although these approaches commonly permit identification of melanomas when they are in situ or thin, it is not known whether they improve survival. In addition, concern remains that visual inspection alone, even for very experienced dermatologists, is inadequate to diagnose all melanomas when they are still curable. Thus, substantial effort is in progress to develop more sensitive and specific diagnostic tools than visual inspection alone. One that is employed routinely in many practices is dermoscopy, also known as epiluminescent microscopy. This involves use of a handheld microscope at the bedside to examine skin lesions in an oil immersion setting. This appears to improve diagnostic accuracy in experienced hands, and increasing experience has made its use more feasible in general practice, especially with considerations for standardization.56,57 When coupled with the use of a digital camera, the images can be stored and compared over time as well. Computer-assisted digital analysis of these images is also being studied but remains investigational.
Evaluation and management of patients with dysplastic nevus syndrome is complicated by the fact that very few dysplastic nevi will develop into melanoma. Estimates range from a risk of 1 per 1,000 nevi examined in a pigmented lesion clinic being melanoma to 1 per 10,000 nevi becoming melanoma per year.56,57 Recommendations for management of dysplastic nevi include those from the Melanoma Working Group in the Netherlands and by a National Institutes of Health Consensus Conference.58
It is tempting to consider excision of all dysplastic nevi. Although that remains an option, there is no proof that this will decrease risk. Melanomas may arise de novo in 30% to 70% of cases, and so it is not clear that removal of all suspicious nevi will lead to a meaningful improvement in survival. However, it is certainly appropriate to biopsy any nevus that is suspicious, especially one that is changing.
Testing for Genomic Changes in Melanoma
Understanding the genetic makeup of melanoma has become the cornerstone of advances in the management of advanced disease, and it is likely to have an increasing role in the management of earlier stage melanoma. Genetic analyses can be focused on driver oncogenic events or can provide a broader understanding of the genomic aberrations in the cancer. Their study is becoming a standard of care practice in melanoma.
Commercially available tests identifying the BRAF V600E/K mutation have been approved by the U.S. Food and Drug Administration (FDA) and other regulatory bodies as companion diagnostics for the use of novel BRAF and MEK inhibitors. These assays are frequently based on specific PCR probes labeled with fluorescent tags that bind to wild-type and V600E or V600K mutant BRAF sequences. These assays are performed in sections of formalin-fixed paraffin embedded tissue blocks routinely used for pathologic analyses. As with all techniques used to detect somatic mutations, they are limited by the amount of mutant sequence in the initial sample as well as DNA integrity in the sample, and their ability to detect non-V600E BRAF mutations since the primers used are usually restricted to this particular BRAF mutation. Multiplexed single nucleotide extension assays (i.e., Sequenom [San Diego, CA] or SNaPshot [Vanderbilt-Ingram Cancer Center, Nashville, TN]) evaluate a list of specific base mutations of interest, but do not identify mutations outside the interrogated bases. These techniques are designed for simultaneous interrogation of different point mutations. They are particularly suited for the targeted interrogation of known oncogenes that contain mutation hotspots, such as NRAS, BRAF, and GNAQ/GNA11, being relevant for melanoma.59
Traditional Sanger sequencing has been the gold standard for the detection of point mutations, but it has been shown to have lower sensitivity than the PCR-based assays, thereby leading to a higher frequency of false negative results. Pyrosequencing provides information from the sequencing 300 and 500 nucleotides at a time, resulting useful for the analysis of mutations clustered in a small gene region. It is a highly sensitive technique, being able to detect mutant DNA when only 5% of the total sample is from the cancer tissue.
Copy number analyses have been very useful in the discovery and description of genes and pathways involved in melanoma pathogenesis. Initially, probe sequences were derived from bacterial artificial chromosomes using array comparative genomic hybridization. More recently, single nucleotide polymorphism-based arrays have been introduced. But currently the approach of choice for the analysis of the DNA alterations in melanoma at the genome level is massively parallel sequencing techniques. These techniques enable the sequencing of exomes and entire genomes of tumor samples (compared to normal DNA from the same patient), with the simultaneous sequencing of a large number of genes and determination of mutations, genetic alterations, and copy number changes. The price and complexity of this type of analysis has rapidly improved, making it feasible to use beyond research studies. Limited panels performing next generation sequencing in what have been called “actionable” genes have been implemented for clinical use. These provide information based on sequencing data of 200 or so genes for which the available literature suggests that they could provide information which may be interpretable to decide on treatment options, in particular in terms of clinical trial participation with new targeted agents.60
A clinically applicable approach to genetic testing of melanomas is first performing a targeted testing for the mutation status of BRAF, NRAS, and KIT in cutaneous and mucosal melanoma samples before pursuing alternative mutation interrogation with higher throughput approaches. Next-generation sequencing may be applicable in situations where known mutations are not identified, and the identification of additional genetic mutations is needed.
DIAGNOSIS OF PRIMARY MELANOMA
Characteristics of Primary Melanoma
The classic appearance of primary cutaneous melanoma is summarized by the mnemonic ABCD for asymmetry, border irregularity, color variation, and diameter >6 mm (see Fig. 38.3). Because melanomas arise from melanocytes, which contain the melaninsynthetic pathway, melanomas classically are distinguished by their pigmentation. Melanomas may have shades of brown, black, blue, red, and white. However, there is a wide range in the appearance of melanomas. Some melanomas are pitch black. Others are shades of brown. Some have no visible pigment and appear skin-colored. Still others have a red color only. When melanomas have all of the classic ABCD features, they are typically easy to diagnose. However, those melanomas that lack some of these features can be difficult to diagnose. In addition, in patients with large numbers of atypical nevi, which may also have ABCD features, this mnemonic is often inadequate to aid in early diagnosis. The other important findings that may aid in early diagnosis are a change in a lesion over time or new development of a skin lesion. These warrant evaluation, and in high-risk patients there should be a low threshold for biopsy. In addition, some dermatologists recommend considering the “ugly duckling” sign: A lesion that stands out as different from the patient’s other nevi should be evaluated and possibly biopsied.61 This can be particularly helpful in a patient with a large number of clinically atypical nevi. Both of these approaches may help to identify amelanotic (nonpigmented) melanomas, which often do not meet the ABCD criteria. Some melanomas are not diagnosed until they become symptomatic, and whereas awareness of the symptoms of bleeding, itching, pain, and ulceration are worth noting, these usually connote deep vertical growth and are hallmarks of a late diagnosis, not an early one.
Biopsy
Biopsy of a suspicious skin lesion is necessary for an accurate diagnosis and for optimal staging. The correct way to perform such a biopsy is to make a full-thickness biopsy of the entire lesion, with a narrow (1 to 2 mm) margin of grossly normal skin. The depth of excision should include the full thickness of dermis and thus should extend into the subcutaneous tissue, but it does not need to include all of the subcutaneous tissue except in very thin patients or patients with very thick polypoid lesions that may go deep into the subcutis. This allows assessment of the architecture of the lesion, which is critical for differentiation of melanoma from Spitz nevus, and it permits an accurate measure of tumor thickness, which is critical for prognosis and affects the surgical treatment recommendations. Of importance, desmoplastic melanoma often arises from LMM and is difficult to diagnose both clinically and histologically. Shave biopsies of these lesions can often lead to failure to appreciate the desmoplastic melanoma in the dermis and may substantially delay diagnosis.
For some large lesions (e.g., >2 cm diameter) in cosmetically sensitive locations (e.g., face or genitalia), there may be a rationale for an incisional biopsy, but that also should be performed as a full-thickness skin biopsy. Ideally, it should include the most suspicious area of the lesion and also should include, if possible, a portion of the edge of the lesion where it transitions to normal skin to enable assessment of the junctional change. The incisional biopsy may be an elliptical incision or it may be a full-thickness 4- to 6-mm punch biopsy. Punch biopsies are problematic if too small, if they do not include full-thickness skin, if they are crushed during removal, if they are oriented inaccurately in the paraffin block, or if they are too small to include both the edge of the lesion and the most suspicious or most raised part of the lesion.
Orientation of the incision used for an excisional biopsy should be considered in the context of the prospect for the future need for a wider re-excision. On extremities, the incision and scar should be oriented longitudinally rather than transversely, although some exceptions may be considered near joints to avoid crossing a joint. When in doubt about the optimal orientation, it is very reasonable to perform the excisional biopsy as a simple circular excision, leaving the wound open for secondary or delayed primary closure.
Biopsy of subungual lesions is more challenging. The pigmentary changes seen in patients with subungual melanoma usually extend along the length of the nail, but the lesions usually arise at the proximal end of the nail bed. Access to that location often requires removal of all or a large part of the nail. One or more punch biopsies of the base of the nail bed often constitute the most realistic method for obtaining a biopsy of such lesions, and it may need to be repeated to be diagnostic. A punch biopsy tool can remove a circle of the nail, providing access to the nail bed for punch biopsy of the suspicious area.
Melanoma Subtypes: Histologic Growth Patterns
Classically, four main histologic growth patterns are described for melanomas, but two others are also worth mentioning.
Superficial Spreading Melanoma
The most common type is superficial spreading melanoma, which accounts for about 70% of primary cutaneous melanomas (see Fig. 38.3C). It is typical for the trunk and extremities, except on acral sites. It is associated with pagetoid growth of atypical melanocytes in the epidermis. Superficial spreading melanoma is commonly associated with sun exposure.
Nodular Melanoma
Nodular melanomas lack an RGP, may be nonpigmented, and commonly are diagnosed when relatively thick. Thus, these carry the worst prognosis of the various subtypes of melanoma. They account for about 20% of cutaneous melanomas. By definition, nodular melanomas are in VGP when recognized.
Acral Lentiginous Melanoma
ALMs account for <5% of melanomas.62 They are typically found on acral sites (subungual, palmar, plantar) and on mucosal surfaces (anorectal, nasopharyngeal, female genital tract). ALM occurs across all races and ethnicities. Its etiology is likely independent of UV light exposure. Because other cutaneous melanomas are uncommon in African, Asian, and Hispanic populations, ALMs on acral sites are proportionately more common in these populations than in fair-skinned whites. ALM is typically associated with a prolonged RGP before vertical growth; however, its locations make it harder to diagnose than other forms of melanoma. Subungual lesions can be detected by linear pigment streaks arising from the base of the nail, but these are not always evident. They can be confused with subungual hematomas, which can lead to diagnostic delay. When there is a question of whether a pigmented subungual lesion may be melanoma or a hematoma, the location of the pigment can be marked and then followed over a short interval (e.g., 3 weeks), during which time a hematoma should move toward the end of the nail, but a melanoma should not.
Subungual melanomas can also present with breakage of the nail or a nonpigmented thickening or drainage, and these are often confused with chronic fungal infections. Any concerning pigmented subungual lesion should be biopsied, but it is sometimes challenging and requires splitting or removing part of the nail. A punch biopsy near the nail bed matrix is often appropriate. In addition, when there is spontaneous chronic inflammation or breakage of the nail, biopsy for melanoma should be considered, even in the absence of pigmentation.
Lentigo Maligna Melanoma
LMMs typically occur in older individuals, in chronically sun-damaged skin, and commonly on the face. They tend to have shades of brown or black, whereas the red and blue colors seen in other melanomas are not typical of LMM. They may also develop areas of regression manifested by depigmentation of part of the lesion. Overall, LMMs account for about 10% to 20% of melanomas in the National Cancer Database experience,1 47% of melanomas of the head and neck, and only 2% of melanomas of other regions.62 LMMs usually have an extensive RGP that extends for many years before developing invasion. When melanoma is just in situ, this RGP portion is called lentigo maligna or Hutchinson freckle, as opposed to LMM. These are not to be confused with the benign pigmented macule, lentigo. Lentigo malignas evolve a VGP to become invasive LMMs at a rate estimated to be between 5% and 33%.63 LMMs are commonly diagnosed as thin lesions. However, more substantial vertical growth can occur, as seen in Figure 38.3A.
Lentiginous Melanoma
Early RGP melanomas sometimes are difficult to classify into the typical patterns of lentigo maligna, superficial spreading melanoma, or ALM. A report defined a distinct entity of lentiginous melanoma. Its features include diameter ≥1 cm, elongated and irregular rete ridges, confluent melanocytic nests and single cells over a broad area of the dermal/epidermal junction, focal pagetoid spread, cytologic atypia, and possible focal dermal fibrosis.64 Over time, this may represent a growing proportion of melanomas that have traditionally been grouped as superficial spreading melanoma, lentigo maligna, ALM, or unclassified melanomas.
Desmoplastic Melanoma
Desmoplastic melanoma is an uncommon form of melanoma, histologically manifest by dermal melanocytes in a dense stromal response. These lesions are usually nonpigmented and usually have lost the melanin production pathway. They usually stain negative for MART-1/MelanA, gp100, and tyrosinase, but they do stain for S100. The lack of pigmentation and the dense stromal response often interfere with clinical and histologic diagnosis. It occurs most commonly in the head and neck, but it may occur in other body sites.65 Desmoplastic melanoma may appear de novo as a nonpigmented skin papule or as a dermal/VGP component arising from a preexisting lentigo maligna or other pigmented junctional lesion. Desmoplastic melanomas may have neurotropic features and have been associated with a high rate of local recurrence.66 However, recent reports suggest that if adequate margins are taken, the risk of local recurrence is low.
The overall mortality risk for desmoplastic melanomas is comparable to that of other invasive melanomas of similar depth of invasion.67 Multiple studies support the contention that desmoplastic melanomas have a significantly lower risk of nodal metastases than other melanomas,68,69,70,71,72 with only 1.4% sentinel node positivity among 155 patients with pure desmoplastic melanoma, compared with 18.5% in those with mixed desmoplastic melanoma.67,68,71,72 There has been a debate about whether to abandon histologic staging of regional nodes in patients with desmoplastic melanoma.69 It may be appropriate to consider a higher threshold for performing sentinel node biopsy (SNBx) in patients with pure desmoplastic melanoma, but there is no consensus on this question.
Prognostic Factors for Primary Melanomas
The best predictor of metastatic risk is the depth of invasion, measured with an ocular micrometer, from the granular layer of the skin to the base of the primary lesion. This was originally described by Breslow73 and remains an important factor in staging and prognostic stratification. However, many other histologic and clinical features have relevance for estimating the risk of future metastasis and mortality. These include age, angiolymphatic invasion, mitotic rate, gender, and body site.
Depth of Invasion
Breslow thickness is the depth of invasion measured from the granular layer of the epidermis to the base of the lesion. Melanoma cells involving adnexal structures are considered junctional and are not included in the Breslow depth. The current melanoma staging system of the American Joint Committee on Cancer (AJCC) identifies tumor (T) stage based on Breslow thickness such that T1 lesions are <1 mm thick, T2 lesions are 1 to 2 mm thick, T3 lesions are 2 to 4 mm thick, and T4 lesions are >4 mm thick.74
Clark et al.75 defined depth based on the layer of skin to which the melanoma has invaded. Clark level I melanomas are melanomas in situ, limited to the epidermis or dermal/epidermal junction. Clark level II melanomas invade into the superficial (papillary) dermis, and these are usually RGP lesions. Clark level III melanomas fill the papillary dermis. Clark level IV melanomas invade into the deep (reticular) dermis and have significant metastatic risk. Clark level V melanomas are uncommon and contain invasion into the subcutaneous fat.
It has become apparent that Clark level does not add much additional prognostic value to Breslow thickness and has been removed from the 2010 version of the AJCC staging system.74 Breslow thickness has an effect on survival, local, regional, and systemic recurrence rates, and that association is continuous, without any apparent breakpoints. Although the staging system requires categorization of thickness ranges, the continuous nature of the risk association should be kept in mind. Thickness is considered in defining the margins of excision for primary melanomas.76,77
Ulceration
Ulceration of the primary lesion has been identified as an important negative prognostic feature76 and is incorporated in the current staging system such that T1a, T2a, T3a, and T4a melanomas are nonulcerated, and T1b, T2b, T3b, and T4b melanomas are ulcerated. In an analysis of prognostic features in a large multicenter database, the prognosis of an ulcerated lesion was comparable to that of a nonulcerated lesion one T level higher. Thus, the overall stage assignment groups ulcerated lesions with nonulcerated lesions one T level higher (e.g., T2b and T3a are both stage IIA). The staging system is summarized in Tables 38.1 and 38.2 and is described in detail elsewhere.74
Patient Gender and Skin Location of Primary Melanoma
The incidence of melanoma is higher for men than women overall, but in adolescents and young adults it is more common in women.25 Furthermore, for essentially all patient subgroups, the prognosis is better for women than men. Thus, among patients with stage III and IV melanoma, men outnumber women approximately 1.5:1. Women are more likely to have melanomas on the extremities, whereas men are more likely to have melanomas on the trunk and head and neck. The clinical outcome for patients with melanomas on extremities is better than that for patients with truncal or head-and-neck melanomas; thus, the prognostic impact of gender is difficult to distinguish from the impact of tumor location. There may still be, however, a prognostic benefit for female gender independent of tumor location.76,78 In addition, location of tumors has prognostic relevance in that head-and-neck melanomas have poorer prognosis than trunk or extremity melanomas, and melanomas on acral sites have poorer prognosis than other extremity melanomas.78,79 A particular location associated with poor prognosis is the mucosal melanoma. Anorectal, female genital, and head-and-neck melanomas of mucosal origin have a mortality risk of 68% to 89% over 5 years.1,79,80
Patient Age
The impact of age on prognosis is confusing. There is a greater risk of lymph node metastasis in young patients at the time of SNBx,81 especially for patients younger than age 35 years, but the melanoma-associated mortality risk increases with age for all thickness ranges.1,76 This paradox has not been explained. It suggests a possible age-specific curative potential for patients with micrometastatic nodal disease. Alternatively, it is worth considering that the attribution of mortality to melanoma progression is not always straightforward. Older patients have other competing causes for death that could lead to earlier mortality in the presence of metastatic disease. Nonetheless, age does appear to have independent prognostic significance for patients with melanoma.
Growth Pattern
Overall, nodular melanomas have the worst prognosis, associated with their diagnosis at a thicker stage. Lesser risk is associated with ALM, superficial spreading melanoma, and LMM, in that order, all associated with decreasing average Breslow thickness. Generally, the histologic growth pattern of melanoma has little prognostic relevance when Breslow thickness is taken into account. The VGP component appears to be the component of melanoma that determines metastatic risk, and these VGP components are similar, independent of the growth phase in the RGP component. LMMs are a possible exception, in that they appear to have a better prognosis than other histologic types, independent of thickness. Desmoplastic melanoma, superficial spreading melanoma, LMM, and ALM have comparable prognosis, for distant metastases and survival, when stratified by thickness.68,81
Mitotic Rate
It is reasonable to expect that the growth rate of melanomas is linked to the rate of tumor cell division. Accordingly, mitotic rate in the dermal component has been identified as a negative prognostic feature, especially with six or more mitoses per square millimeter.81,82 Similarly, dermal expression of Ki67, a molecular marker of proliferation, is associated with greater risk of metastasis.83 For thin melanomas, the presence of any mitotic figures has been associated with metastatic risk, whereas the absence of dermal mitoses is associated with an excellent prognosis.84 The current staging system incorporates mitotic rate of ≥1/mm2 in differentiating low-risk thin melanomas (T1a) from higher-risk thin melanomas (T1b), and data used to define the current staging system identify increasing risk with increasing mitotic rate for all thicknesses.74 Increased mitotic rate is associated with a poorer prognosis across all thickness ranges, but is not yet incorporated formally in the staging system beyond the current cutoff of 1/mm2 for thin lesions.74,85,86
aClinically undetectable nodes are those diagnosed only with sentinel node biopsy or elective lymphadenectomy, and lacking gross extracapsular extension. They are referred to also as micrometastases, but this definition differs from the pathologist’s definition of a micrometastasis as one that is <2 mm in diameter.
bClinically detectable nodes are also referred to as macrometastases, but this is a different definition than the pathologist’s definition based on a diameter >2 mm. Patients with gross extracapsular extension are also considered to have macrometasetasis.
Modified from Edge S, Byrd DR, Compton CC, et al., (eds.). AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010.
Other Prognostic Factors
There is also evidence, and biologic rationale, that angiolymphatic invasion has negative prognostic significance,81 and that microscopic satellites are associated with poorer prognosis. Satellitosis is incorporated in the current staging system74 but will be considered separately because it defines the patient as stage III and thus goes beyond assessment of risk factors of the primary lesion alone.
Unresolved Issues in Melanoma Staging
The AJCC staging system is evidence-based and accounts for several important clinical and histopathologic findings. However, several clinical settings are not fully addressed by the AJCC staging system. These include the following.
TABLE 38.2 Pathologic Stage Grouping for Cutaneous Melanoma
aClinical staging includes microstaging of the primary melanoma and clinical-radiologic evaluation for metastases. By convention, it should be done after complete excision of the primary melanoma with clinical assessment for regional and distant metastases.
bPathologic staging includes microstaging of the primary melanoma and pathologic information about the regional lymph nodes after partial or complete lymphadenectomy. Pathologic stage 0 or stage IA tumors are the exception; they do not require pathological evaluation of the lymph nodes.
Modified from Edge S, Byrd DR, Compton CC, et al., (eds.). AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010.
Positive Deep Margin on Biopsy
When a primary melanoma is diagnosed by shave biopsy, and the tumor extends to the deep margin, it is presumed that the melanoma was deeper than the original measured biopsy depth. Sometimes, on wide local excision there is residual melanoma with a greater depth than on the original biopsy. In that setting, it is appropriate to define the T stage based on the latter depth of invasion. However, in many cases, the wide excision does not reveal any more melanoma, or may reveal tumor that is more superficial. It is generally assumed that in those cases, any residual melanoma at the deep margin may have been destroyed by inflammatory changes after the biopsy. One approach for defining T stage in that setting is to call it TX. The other is to use the T stage of the original depth, even though that is incomplete. The latter has the advantage of distinguishing thin melanomas (e.g., a clinically thin melanoma with thickness <1 mm) from a thick melanoma (e.g., a 5-mm melanoma on shave biopsy, with positive deep margin). Thus, use of TX results in substantial loss of information for patients and their clinicians.
Local Recurrence After Original Incomplete Excision
Some patients present with melanoma after excisional biopsy or destruction (e.g., cryotherapy) of a pigmented skin lesion that was believed to be benign (clinically or histologically) on initial review. When such a lesion recurs and is found to contain melanoma, re-review of the original biopsy is appropriate, if available. Staging of such recurrent melanomas, when the original lesion was not known to be melanoma, is not well addressed.
Skin or Subcutaneous Lesion Without Junctional Involvement and Without Known Primary Melanoma
This is addressed later in this chapter. Cutaneous or subcutaneous nodules that occur in the absence of junctional melanocytic change, and in the absence of any other known primary, are among the most interesting presentations of melanoma. They may be intransit metastases from primary melanomas that spontaneously regressed (stage IIIB), primary melanomas that arose from dermal nevi or that persisted in the dermis after arising from a partially regressed primary melanoma (stage IIB), or a distant metastasis from an unknown primary melanoma (stage IV, M1a). A review of experience with these lesions at the University of Michigan suggests that they behave more like primary tumors arising in the dermis or subcutaneous tissue.76 In the current staging system, these are considered stage III.
GENERAL CONSIDERATIONS IN CLINICAL MANAGEMENT OF A NEWLY DIAGNOSED CUTANEOUS MELANOMA (STAGE I-II)
Most melanomas present as clinically localized lesions without clinical or radiologic evidence of metastatic disease. Nonetheless, some of these patients have occult metastases, and the definitive surgical management includes both therapeutic resection and pathologic staging evaluation for regional metastases. The vast majority of primary melanomas are diagnosed on histologic assessment of skin biopsy performed by a dermatologist or a primary care practitioner. The patient then presents to a surgeon or other physician for definitive treatment.
Clinical Evaluation and Radiologic Studies for Patients with Clinical Stage I-II Melanoma
In patients with clinically localized melanoma, there is a wide range of clinical practice in the appropriate radiologic staging studies to be performed. Certainly all patients with such disease should have a complete history and physical examination, with attention to symptoms that may represent metastatic melanoma, including headaches, bone pain, weight loss, gastrointestinal symptoms, and any new physical complaints. Physical examination should carefully assess the site of the primary melanoma for clinical evidence of persistent disease and should evaluate the skin of the entire region (e.g., whole extremity or quadrant of torso, or side of the face) for dermal or subcutaneous nodules that could represent satellite or in-transit metastases. Biopsy should be done for any suspicious lesions and with a very low threshold for biopsy. In addition, physical examination should include thorough evaluation of both the major regional nodal basins (e.g., epitrochlear and axillary for a forearm melanoma) and also any atypical lymph node locations, such as the triangular intermuscular space on the back for upper back primaries.
There is a great deal of uncertainty and debate about appropriate initial staging studies. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) from 2013 recommend no staging radiographs or blood work for melanoma in situ, and recommend imaging for low-risk thin melanomas (stage IA) “only to evaluate specific signs or symptoms.” For clinical stage I-II, no other imaging is recommended. For stage III melanoma, consideration of imaging is recommended, to include chest radiograph (CXR), computed tomography (CT) scans, or positron emission tomography (PET)/CT scans, with consideration of magnetic resonance imaging (MRI) of the brain, and other imaging is suggested only as clinically indicated. More complete staging studies are suggested for stage III melanoma.87
CXR for asymptomatic patients with a new diagnosis of clinically localized melanoma yielded suspicious findings in 15% of patients, of whom only 0.1% had a true unsuspected lung metastasis.88 In a similar study, the yield of true positive CXR was 0% of 248 patients.89 In patients with stage IIB melanoma, initial staging CT scans identified occult metastasis that changed management in 0.7% of patients.90 Even in patients with positive SNBx, staging PET scan identified no melanoma metastases in 30 patients, even though there were lymph node metastases in 16% of cases.91 In patients with clinical T1b-T3b melanomas, true positive rates for all imaging studies was 0.3%, and falsepositive rates were 50% to 100% for CXR, 88% for CT and PET/CT scans.92 Thus, there is a large body of data that argues that CXR, CT, and PET/CT are all of little or no value in initial staging of melanoma stage 0-IIIA.
PET with fluorodeoxyglucose (FDG) has a role in staging patients with advanced melanoma,93 but its role in earlier-stage disease is less clear both because it is expensive and because it is associated with substantial radiation exposure. In one study, patients with clinically localized melanomas >1 mm thick, with local recurrence, or solitary in-transit metastases, FDG-PET scanning was performed prior to sentinel node biopsy. Sensitivity for detection of sentinel nodes was only 21%, although specificity was high (97%). In addition, 21% of patients had PET evidence of metastases, but none was confirmed by conventional imaging at that time, and the sensitivity for predicting sites of future disease recurrence was only 11%. Overall sensitivity for detecting occult stage IV disease was only 4%, and this is not recommended for initial staging.94 These findings are similar to other experiences with PET imaging for intermediate-thickness melanomas.95,96
Also, some clinicians send blood for a complete blood count, for serum chemistries, including liver function tests, and for a lactate dehydrogenase (LDH) level, especially as they may be useful prior to surgery under general anesthesia. These also are of low clinical yield in terms of the melanoma but may detect unappreciated concurrent illness that may affect therapeutic decisions, including preoperative assessment. Specifically, if there is microcytic anemia, it should be worked up, with the differential diagnosis to include gastrointestinal metastasis of melanoma. Elevated LDH should prompt a more extensive staging workup, and elevated liver function tests should prompt a hepatobiliary ultrasound or CT scan unless there is another known explanation.
Wide Local Excision for Clinical Stage I-II Melanoma: General Considerations
Wide excision of the primary melanoma is performed to provide local control. Multiple randomized, prospective clinical trials support current recommendations for the extent of the margins of resection. The wide excision also provides an opportunity to evaluate the tissue adjacent to the primary lesion for microscopic satellites, which, if present, have clinical and prognostic significance.
There has been considerable debate about the appropriate margins of excision for primary melanomas, and it is helpful to understand the evolution of thought and data about this topic. In the early 1900s, melanoma was a rare disease, and when it was diagnosed, it was often locally advanced. Surgical resection was often associated with recurrence disease, and there were no guidelines for appropriate and successful surgical management of the primary lesion. In 1907, Handley reported a study that involved histologic examination of tissue sections taken at varied distances from the primary melanoma in a human tissue specimen that he obtained from a patient with a large primary melanoma. In that study, he found microscopic evidence of melanoma cells as far as 5 cm from the primary tumor. He recommended wide re-excision of melanomas with a measured margin of 5 cm from the primary lesion. This recommendation became standard management for melanoma for many decades, with patients typically undergoing radical resections requiring skin grafts ≥10 cm in diameter.
As melanoma became a more frequent diagnosis, there was greater awareness of it, and lesions were often diagnosed at an earlier (thinner) stage. In addition, these large re-excisions usually contained no detectable melanoma cells separate from the primary lesion. These observations, and concern for the morbidity of large resections and skin grafts, led to a questioning of the need for 5-cm margins of resection. It is ironic that the origin of this aggressive resection practice was based on data from a single patient in a single study; however, limiting the margins of excision has required multiple large, randomized, prospective trials. These trials are summarized in Table 38.3 and are detailed in the follow sections.
TABLE 38.3 Prospective Randomized Clinical Trials of Melanoma Excision Margins
Clinical Trial
N
Thickness Ranges (mm)
Margins-Study Groups (cm)
Local Recurrence
Disease-Free Survival
Overall Survival
World Health Organization Melanoma
Program Trial No. 10
612
0-2
1 vs. 3-5
None for 0-1 mm with 1 cm margins; for 1-2 mm, more local recurrences with 1 cm margins (NS)
—
No difference
French
▪ Cooperative
▪ Surgical trial
337
0-2
2 vs. 5
No difference; 10-y DFS 85% and 83%, respectively
No difference; 10-y survival 87% and 86%, respectively
Swedish
▪ Cooperative
▪ Surgical Trial
989
0.8-2
2 vs. 5
<1% overall
No difference; relative hazard rate for 2 cm margin 1.02 (0.8, 1.3)
No difference; relative hazard rate for 2 cm margin 0.96 (0.75, 1.24)
Intergroup
▪ Melanoma trial
740
1-4
2 vs. 4
0.4% (first, recurrence) 0.9% (first recurrence), 2.1% ever for 2 cm margins; 2.6% ever for 4 cm margins
—
10-y disease-specific survival 70% for 2 cm margins; 77% for 4 cm margins (p = 0.074, NS)
British Cooperative
▪ Group trial
900
≥2
1 vs. 3
(Locoregional = local + in-transit + nodal) Increase with 1 cm margin (hazard ratio 1.26, p = 0.05)
—
Similar; trend to better survival with 3 cm margins, p >0.1 (NS)
DFS, disease-free survival; NS, not significant.
CLINICAL TRIALS TO DEFINE MARGINS OF EXCISION FOR PRIMARY CUTANEOUS MELANOMAS
The World Health Organization (WHO) Melanoma Program Trial No. 10 randomized 612 melanoma patients with melanomas ≤2 mm in thickness to excision margins of 1 cm versus 3 to 5 cm.97,98 Patients were stratified into two subgroups: Breslow depth <1 mm versus 1 to 2 mm. There were no differences in survival rates or in rates of distant recurrences with 1-cm margins versus 3- to 5-cm margins with follow-up beyond 15 years.99 There were more local recurrences for the group with 1-cm margin (eight versus three patients), but this was not a significant difference. There were no local recurrences for melanomas <1 mm thick treated with 1-cm margins. The lack of local recurrences with thin melanomas (<1 mm) after 1-cm margins of excision support this as a standard excision margin for T1 melanomas. The numerically slightly higher (but statistically insignificant) local recurrence risk with thinner margins for T2 melanomas has left questions about the appropriate margin for thicker lesions.
French and Swedish Cooperative Surgical Trials
The French Cooperative Group randomized 337 patients with melanomas up to 2 mm in thickness to 2- or 5-cm margins.100 Ten-year disease-free survival rates were 85% and 83%, respectively, and tenyear overall survival (OS) rates were 87% and 86%, respectively.100 The Swedish Melanoma Study Group randomized 989 patients with primary melanoma 0.8 to 2 mm thick on the trunk or extremities to 2- or 5-cm margins. Local recurrences were observed in only eight patients overall (<1%). In a multivariate Cox analysis, estimated hazard rates for OS and recurrence-free survival for those with 2-cm margin were 0.96 (95% CI, 0.75 to 1.24) and 1.02 (95% CI, 0.8 to 1.3), respectively, compared with the 5-cm margins.101 Both of these studies support 2-cm margins as adequate for melanomas up to 2 mm thick and find no added benefit to 5-cm margins.
Intergroup Melanoma Trial
The Intergroup Melanoma Surgical Trial addressed the question of surgical margins in 740 patients with intermediate-thickness melanomas (1.0 to 4.0 mm thick) randomized to either 2- or 4-cm margins.102 Patients were stratified by tumor thickness (1 to 2 mm, 2 to 3 mm, and 3 to 4 mm), anatomic site (trunk, head and neck, and extremity), and ulceration (present or absent). Patients with melanomas on the head and neck or distal extremity were not randomized for margin of excision because 4-cm margins are not readily performed in such locations. Thus, 468 patients (group A) were actually randomized for margin of excision. All patients were also randomly assigned to undergo either an elective lymph node dissection (ELND) or observation after wide local excision, and this component of that study is discussed separately.102 Among the 468 patients in group A (randomly assigned to excision with 2- versus 4-cm margins), only 3 (0.6%) experienced a local recurrence as the first site of failure, and 11 (2.3%) had local recurrence overall.102 Among the 272 patients in group B (nonrandomly assigned to excision with a 2-cm margin), a higher rate of local recurrence was observed, with 3.7% having a local recurrence as a first recurrence and 6.2% overall experiencing a local recurrence during the course of their disease.102 Among these 468 patients in group A, the incidences of local recurrence as first relapse were 0.4% versus 0.9% for 2- and 4-cm margins, respectively, and the incidences of local recurrence at any time were 2.1% versus 2.6%, respectively. In addition, the time to local recurrence and the median survival after local recurrence were unaffected by the extent of the margin. Ten-year disease-specific survival rates for the two groups were 70% and 77% for 2- and 4-cm margins, respectively (p = 0.074, not significant). Thus, this study supports a 2-cm margin as adequate for melanomas 1 to 4 cm thick, and this was associated with rates of local recurrence (as first recurrence) well <1%. Multivariate analysis of data from this study further supported the lack of benefit of wider margin of excision for local control and identified ulceration of the tumor and head-and-neck location only as significant negative prognostic features.
British Cooperative Group Trial
The British randomized trial compared 1- versus 3-cm margins of excision in patients who had cutaneous melanomas ≥2 mm thick (T3, T4).103 Nine hundred patients with T3 and T4 melanomas were accrued, of whom 25% had T4 melanomas. It is the only randomized trial evaluating margins of excision that included patients with T4 melanomas. Patients with melanoma on head and neck, hands, or feet were excluded. No patients had any surgical procedure to stage the regional nodal basins (sentinel node biopsy or ELND) or systemic adjuvant therapy. The trial was stratified according to tumor thickness (2 to 4 mm versus >4 mm). There were few local recurrences; local recurrences and in-transit metastases were not statistically more frequent in the 1-cm margin group. Locoregional recurrences were defined broadly to include local, in-transit, or regional nodal recurrences. Using that definition, a 1-cm margin of excision was associated with a significantly increased risk of locoregional recurrence (hazard ratio [HR], 1.26; p = 0.05). Overall survival was comparable for the two groups (p = 0.6); there was a nonsignificant trend toward higher death rate in the group with 1-cm margins (128 versus 105 deaths; HR 1.24, p = 0.1). This study has been controversial, and its relevance to current practice is questioned because of the lack of surgical staging of the regional nodes, but it does challenge the safety of 1-cm margins for melanomas >2 mm thick.103 These results support excision >1 cm for thicker melanomas. The data from the Melanoma Intergroup study support 2-cm margins for melanomas 2 to 4 mm thick. No data have formally compared 2-cm margins with 3-cm margins for T4 melanomas.
SURGICAL STAGING OF REGIONAL NODES
Thin and RGP melanomas are commonly cured by excision alone; however, thicker melanomas may have metastatic potential. Initial management includes an assessment for metastases and consideration of treatment options that may be beneficial in providing regional control and systemic control. Melanoma may metastasize by lymphatic or hematogenous routes. Usually, lymphatic dissemination presents earlier than hematogenous dissemination. Thus, emphasis is placed on staging the regional nodes in patients with melanoma. The finding of lymphatic metastases is associated with a higher risk of systemic disease. Another potential benefit of staging the regional nodes is to select patients for curative resection. There are substantial data on this issue that bear on the current recommendations for surgical staging of nodes, and these are summarized here.
Lymphatic anatomy is variable and is poorly understood in comparison to venous and arterial anatomy. Classic work by Sappey defined aspects of lymphatic drainage patterns from skin and defined the skin regions that typically have lymphatic drainage to major nodal basins. More recently, lymphoscintigraphy has permitted mapping the actual lymphatic drainage patterns from the skin at the site of the primary melanoma. This sometimes identifies lymphatic drainage that differs from Sappey’s predictions.
In the past, the standard recommendation was to perform ELNDs for melanomas of intermediate thickness (1 to 4 mm). Despite some retrospective data supporting this approach,104 subsequent retrospective and prospective studies have failed to show a significant survival advantage to routine ELND.105,106,107 In the early 1990s, a new procedure was developed and popularized for surgical staging of node-negative primary melanomas, which is called intraoperative lymphatic mapping and sentinel lymph node biopsy. This approach has become routine practice for melanoma management.
The concept and method for SNBx was originally developed by Cabanas108 for management of penile carcinomas, but it was not pursued extensively. The initial experience with lymphatic mapping and SNBx for melanoma was the work of Morton et al.109 at the University of California Los Angeles and the John Wayne Cancer Institute. They injected a vital blue dye (isosulfan blue) intradermally and found that this stained the draining lymphatics and stained, in turn, the first node(s) into which these lymphatics empty. This was validated in human clinical experience and it was rapidly adopted as an effective way to identify the first lymph node(s) to which the melanoma drains.110 The sentinel node(s) serve as sentinels for the remainder of the node basin. Lymphatic mapping permits identification of the specific nodes that drain the relevant area of skin, and so these nodes (typically one or two nodes) can be excised for detailed histopathologic assessment while sparing the remaining nodes in that basin, which are critical for drainage of other skin areas, thus minimizing morbidity, in particular lymphedema.
Lymphoscintigraphy has been coupled with the blue dye injection to support identification of the sentinel node(s), using handheld probes for detection of γ radiation emitted by technetium-99 (99Tc), the radionuclide commonly used in lymphoscintigraphy. Most surgical oncologists performing SNBx use a combination of radionuclide injection several hours preoperatively (in the nuclear medicine suite, up to 1 mCi of 99Tc) and intraoperative intradermal injection of isosulfan blue dye (up to 1 ml) a few minutes prior to the incision. The injection of radiocolloid is shown in Figure 38.6. The sentinel node(s) should be both blue and radioactive (“hot”). However, sometimes the blue dye may fail to enter the node in the short interval before the dissection. Alternatively, if the dissection takes longer than anticipated, the blue dye may transit through the node by the time the node is identified. In addition, technical issues may result in the blue dye and radiocolloid being injected in slightly different areas, such that they identify different nodes. The gamma probe is used to guide the dissection to the sentinel node(s), as suggested in Figure 38.7.
Lymphatic mapping and SNBx using both blue dye and radiocolloid increases sentinel lymph node identification rates to 99% compared with 87% with blue dye (p <0.0001).111 However, radiocolloid alone has not been formally compared with radiocolloid plus blue dye. There is substantial multicenter and single-center experience with use of radiocolloid alone, which is associated with successful identification of the sentinel node(s) in >99% of patients and with a mean of approximately two sentinel nodes per patient.112 The effectiveness of blue dye alone is limited because some patients have drainage to lymph node basins that may not be predicted (e.g., drainage from the right upper back to the left axilla) or drainage to atypical nodal basins (e.g., the triangular intermuscular space on the back, epitrochlear or popliteal nodes, or subcutaneous “in-transit” nodes that are outside a traditional nodal basin).113,114 Examples of unusual lymph node locations mapped by lymphoscintigraphy are shown in Figure 38.8. Thus, in the large majority of clinical settings, it is most appropriate to perform radiocolloid lymphoscintigraphy in lymphatic mapping for SNBx of melanoma.
Figure 38.6 Injection of technetium-99 sulfur colloid intradermally near primary melanoma.
Figure 38.7 Schematic of a way to identify and remove the sentinel node using a handheld gamma camera.
In experienced hands, lymphatic mapping should identify a sentinel node in 98% to 100% of cases, and it should be feasible to perform the SNBx with minimal morbidity, on an outpatient basis, and in many cases under local anesthesia with sedation. The early reports of SNBx stress a long learning curve, but as the technology of gamma probes has improved, the technique is less operator dependent. In addition, lymphatic mapping has now been performed long enough that surgical residents trained since the mid-1990s typically have had experience with it for melanoma and for breast cancer. The standard evaluation of a sentinel node includes evaluation of multiple sections of the node, often combined with immunohistochemical staining for melanoma markers (e.g., S100, HMB45, tyrosinase, and/or MART-1/MelanA).
Typical results of SNBx reveal that the rate of positive nodes increases with increasing tumor thickness, as would be expected, from <5% for the thin melanomas that undergo SNBx (e.g., T1b lesions) to approximately 40% for thick melanomas. Current experience with SNBx in most series supports the prognostic value of SNBx in thick melanomas (>4 mm)115 as well as in thinner lesions. When ELND was performed, it was typically recommended only for melanomas 1.5 to 4 mm thick. However, in the Duke experience, the relative risk of distant versus regional metastases is not dramatically higher for thick melanomas, and this supports a clinical approach that includes the potential for curative resection of regional metastases in these cases.105 In addition, the low morbidity of SNBx supports a threshold for SNBx in thinner melanomas than the 1.5-mm criterion that was used for performance of ELND.
The overall rate of positive SNBx in most series (typically for melanomas >1 mm) is in the range of 15% to 25%. The percentage of patients with false-negative SNBx in experienced hands and with use of radiocolloid and the handheld gamma probe, with or without blue dye, is typically in the range of 1.9% to 4%.111 The most rigorous definition of false-negative rate is false negative/(false negative + true positive), and 3% false negative in the setting of 20% true positive represents 13% false-negative rate. False-negative rates have been estimated by seeking nodes containing metastases in the remaining nodal basin after a negative SNBx. In other settings, it is done by defining patients who return with clinically evident nodal metastases after a prior negative SNBx in the same node basin. These may or may not be equivalent. Nonetheless, there is a small percentage of patients who have negative SNBx who later return with nodal metastases in the same nodal basin. Although the procedure is very accurate and does identify the large majority of nodal metastases, it is prudent to follow patients for nodal recurrence even after a negative SNBx.
Lymphatic mapping and SNBx has been applied generally for all cutaneous sites and may also be useful for melanomas of mucous membranes.116 A challenging area for SNBx is the head and neck. In particular, melanomas of the scalp and of the face may drain to parotid nodes or periparotid nodes, for which SNBx is more complex, more technically challenging, and associated with greater potential morbidity. In addition, false-negative SNBx are more common than in trunk and extremity melanomas, occurring in approximately 10% of patients, for a true false-negative rate that may approach 30%. However, in many cases, it can be performed reliably and still has a place in management.
Only gold members can continue reading. Log In or Register to continue