Chapter 19 Congenital Disorders of Lymphocyte Function
Diagnostic Approach to Severe Combined Immune Deficiency
• SCID presents early in life with severe infections of bacterial, viral, or fungal origin.
• Opportunistic infections are common in infants with SCID.
• Respiratory infections, protracted diarrhea, and failure to thrive are typical signs at presentation.
• Lymphopenia is present in 50% to 70% of infants with SCID. Age-specific norms must be used in evaluating the ALC because infants and children have much higher ALCs than adults (3500-13,000 cells/mcL in very young infants versus 1000-2800 cells/mcL in adults).
• T-cell lymphopenia is the hallmark of the disease; abnormalities of the absolute count of B and NK lymphocytes are observed in some forms of SCID. However, T lymphocytes may be present in SCID infants with maternal T-cell engraftment or with hypomorphic mutations in SCID-associated genes that allow residual T-cell development. Thus a normal ALC does not rule out SCID.
• Maternally engrafted T cells proliferate in the infant with SCID in vivo, but the vast majority of the time do not proliferate in vitro when stimulated with traditionally used mitogens such as concavalin A and phytohemagglutinin, as measured by thymidine incorporation. Thus, if SCID is suspected but T cells are detectable, maternal engraftment studies and proliferation to mitogens must be done.
• Universal newborn screening has now been piloted in a growing number of states since 2009. The analyte is detection of TRECs by quantitative polymerase chain reaction. TRECs are high in newly generated T cells and low when T cells are absent or when maternally engrafted T cells are present.
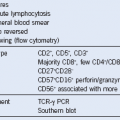
• SCID is genetically heterogeneous. The most common form in Western countries is inherited as an X-linked trait and is T− B+ NK−.
• The lack of all lymphocytes (T− B− NK− SCID) is highly suspicious for the ADA form of SCID in which toxic metabolites result in death of all lymphocytes. Testing for ADA enzyme level is critical because if confirmed to be absent, treatment with PEG-ADA can often result in sufficient reconstitution of T-cell immunity to protect the baby from infection.