CLINICAL PRESENTATION
Part of “CHAPTER 65 – PAGET DISEASE OF BONE“
The localized nature of Paget disease leads to a variable clinical presentation. Frequently, only one or two bones are involved; alternatively, many bones may be affected. The most commonly involved sites include the pelvis, spine, skull, femur, and tibia. The bones of the upper extremities, the clavicles, scapulae, and ribs are somewhat less commonly involved, and the hands and feet are seldom affected. Clinical symptoms and complications of Paget disease depend greatly on the sites of involvement, the relation of pagetic bone to adjacent structures, and the extent of ongoing metabolic activity.
Most patients with Paget disease are asymptomatic, and the diagnosis is an incidental finding, made when either an elevated serum alkaline phosphatase level is discovered or a radiograph showing classic pagetic changes is obtained for some unrelated reason. Other patients have symptoms referable to the skeleton, but these may reflect a range of causes, including problems with the bone itself, joint dysfunction adjacent to pagetic bone, neurologic abnormalities, and changes associated with increased blood flow. Depending on the site of involvement and the nature of the skeletal alterations that are occurring, a simple complaint such as bone pain may be difficult to characterize. For example, patients with skull involvement may describe headaches or tightness across the scalp, or they may note a sensation of warmth, presumably reflecting the increased blood flow through pagetic bone and surrounding soft tissues. A symptom of pain in the back in the setting of one or more enlarged pagetic vertebrae may come from the bone itself, but is probably due to degenerative changes of the joints that are exacerbated by the presence of Paget disease, with or without spinal nerve impingement and muscle spasm. Pagetic involvement of the pelvis or proximal femur may include the hip joint, leading to pain in the groin or in the thigh, often radiating to the knee. This common pattern is a major source of discomfort in patients with Paget disease at this site.
Bone deformity may be the patient’s presenting problem. Enlargement or bowing of the femur or tibia is a readily apparent finding, as are skull enlargement with classic frontal bossing, asymmetry of the pelvic or shoulder girdle areas, and kyphosis (Fig. 65-5). When the femur or tibia on one side of the body has a bowing deformity caused by Paget disease, adjacent joints are subjected to mechanical stresses from the curvature; in addition, the bowed limb is typically shortened, increasing the likelihood of back pain or contralateral joint dysfunction and pain resulting from the abnormal gait. These symptoms are among the most common. As with the skull, a sensation of increased heat in a bowed extremity is a frequently stated complaint. Often this increased warmth is felt by the examiner’s hand.
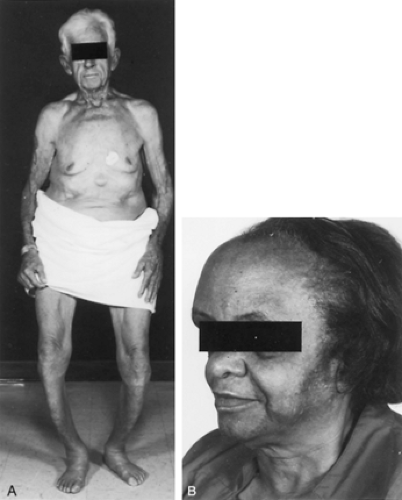 FIGURE 65-5. A, Extensive Paget disease in an elderly man, showing considerable deformity of the lower extremities. Outward bowing of the femoral, tibial, and fibular bones and anterior bowing of the shins (saber shins) are seen. The patient also has thoracic kyphosis. Considerable secondary degenerative arthritis of the knees and hips is present. (The nodule on the abdomen is a sebaceous cyst.) B, Severe pagetic involvement of the skull, showing deformity and enlargement of the frontal bone. The patient complained of a throbbing discomfort of the head, and the overlying skin was very warm.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|


