Chapter 27 Chronic Myeloid Leukemia
Management of the Newly Diagnosed Chronic Myeloid Leukemia Patient
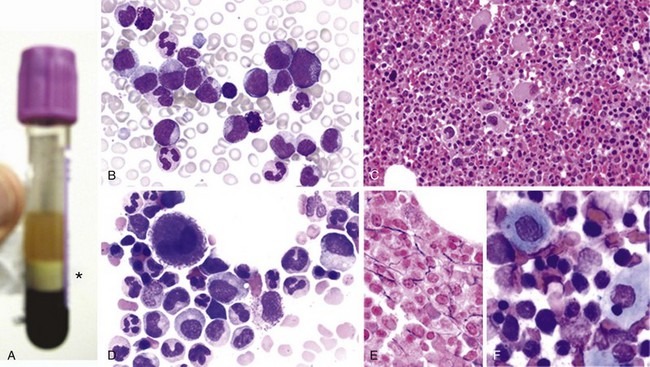
Figure 27-1 CHRONIC MYELOGENOUS LEUKEMIA, PERIPHERAL BLOOD TUBE, AND IMAGES OF BLOOD SMEAR AND BONE MARROW BIOPSY AND ASPIRATE IN CHRONIC PHASE.
Related posts:
 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
Clinical Manifestations and Treatment of Acute Lymphoblastic Leukemia in Children
Approach to Anemia in the Adult and Child
Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 2
Hematologic Changes in Pregnancy
Pain Management and Antiemetic Therapy in Hematologic Disorders
Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
Clinical Manifestations and Treatment of Acute Lymphoblastic Leukemia in Children
Approach to Anemia in the Adult and Child
Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 2
Hematologic Changes in Pregnancy
Pain Management and Antiemetic Therapy in Hematologic Disorders
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


