ADRENAL ADENOMAS
Incidentally discovered adrenal adenomas (incidentalomas) are found in 1% to 4% of the population on CT scans.1 Considerable effort has been devoted to the development of CT and MRI techniques for differentiating benign adrenal tumors from other adrenal masses.
Adrenal adenomas are round or oval, homogeneous masses with a smooth, well-defined margin, and are usually <2 cm in diameter (Fig. 88-2).2 In patients with known extraadrenal cancer, adrenal masses that are >3 cm in diameter or that have irregular margins have a high probability of malignancy.3 Biopsy should be performed.
 FIGURE 88-2. Adrenal adenoma. A homogeneous, oval, 2.5-cm mass with smooth margins is seen in the right adrenal gland (arrow). On this noncontrast CT scan, its attenuation is -3 Hounsfield units. It was an incidental finding in this 40-year-old woman. |
In patients who do not have a known malignancy, an incidentally discovered adrenal mass >5 cm may be an adrenal cancer. This size criterion had a sensitivity of 93% and a specificity of 64% for differentiating adenomas and carcinomas in a series of 210 patients with incidentally discovered adrenal masses.4 Other features suggestive of adrenal carcinoma are central areas of decreased attenuation, calcification, and evidence of hepatic, venous, or nodal spread (Fig. 88-3).5 Note, however, that large, degenerated adrenal adenomas often contain areas of calcification, hemorrhage, or necrosis.5a No universally reliable imaging criteria, other than size, are available for differentiating adrenal adenoma from adrenal carcinoma on CT scans.
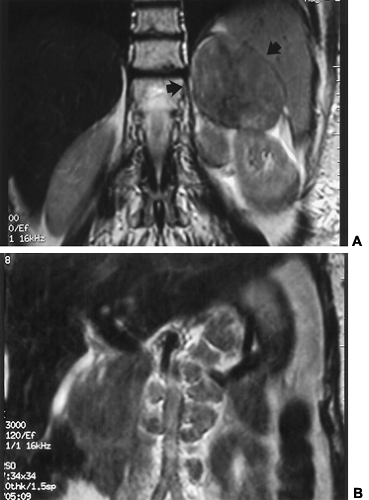 FIGURE 88-3. Adrenal carcinoma. A, The 9-cm mass in the left adrenal gland (arrows) has low signal intensity on this coronal T2-weighted magnetic resonance image and shows some central inhomogeneity. Whatever its imaging characteristics, the tumor’s size alone suggests that adrenal carcinoma should be strongly considered. B, A more anterior coronal image demonstrates paraaortic adenopathy, which supports the diagnosis of adrenal carcinoma. |
Adrenal adenomas, regardless of whether they demonstrate clinical endocrine function, usually contain an abundance of intracytoplasmic lipid; metastases do not.6 Most CT and MRI maneuvers used to diagnose adrenal adenomas are designed to demonstrate or quantify this lipid content. The simplest method is measurement of adrenal attenuation on a CT scan obtained without intravenous contrast material. CT attenuation is measured in Hounsfield units (HU), with water arbitrarily assigned a value of 0 HU. The greater the amount of lipid in an adrenal mass, the lower its attenuation. Some investigators have reported a mean attenuation of 2.5 HU for adrenal adenomas versus 32 HU for other adrenal lesions (see Fig. 88-2),7 and others have found a mean attenuation of 4 HU for adenomas and 37 HU for other adrenal masses.8 Unfortunately, substantial variability exists in the amount of lipid present from adenoma to adenoma; therefore, substantial variability is seen in attenuation as well. Threshold values from 20 HU to 2 HU have been used in the radiologic literature to distinguish between adenomas and other adrenal lesions. With a 20-HU threshold, sensitivity is 88%, but specificity is 84%. If a 2-HU threshold is used, specificity increases to 100%, but sensitivity is only 47%.9 Many centers use a 10-HU cutoff value.10
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


