Chapter 6 Acquired Disorders of Red Cell, White Cell, and Platelet Production

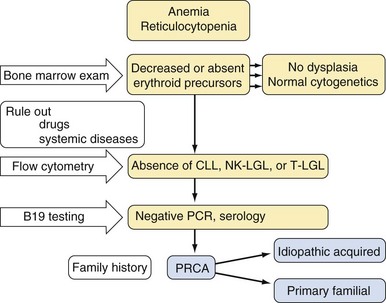
Table 6-2 Classification of Neutropenia
| Congenital | |
| Primary | Autoimmune neutropenia |
| Pure white cell aplasia | |
| Idiopathic | |
| Thymoma | |
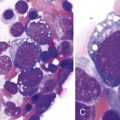
| Hematologic malignancies (e.g., T-LGL leukemia) | |
| Infections/postinfectious | |
| Viral | |
| Measles,53 mumps, roseola,54,55 rubella,56 RSV, influenza57 | |
| Hepatitis A,58 B,58,59 and C60 | |
| CMV,61–63 EBV,64–66 HIV67,68 | |
| Parvovirus69–71 | |
| Bacterial | |
| Tuberculosis72,73 | |
| Brucellosis74–76 | |
| Tularemia77 | |
| Typhoid fever78 | |
| Rickettsial | |
| Rocky Mountain spotted fever79 | |
| Ehrlichiosis80,81 | |
| Fungal | |
| Histoplasmosis82,83 | |
| Parasitic | |
| Malaria,84 leishmaniasis85,86 | |
| Autoimmune conditions (e.g., SLE87,88, RA89) | |
| Drugs and chemicals | |
| Neutropenia associated with immunodeficiency90,91 | |
| Severe nutritional deficiencies92,93 | |
| Neutropenia due to increased margination | |
| Iatrogenic (e.g., hemodialysis94,95) |
CMV, Cytomegalovirus; EBV, Epstein-Barr virus; HIV, human immunodeficiency virus; RA, refractory anemia; RSV, respiratory syncytial virus; SLE, systemic lupus erythematosus; T-LGL, T-cell large granular lymphocyte.
Table 6-3 Drugs Associated With Agranulocytosis
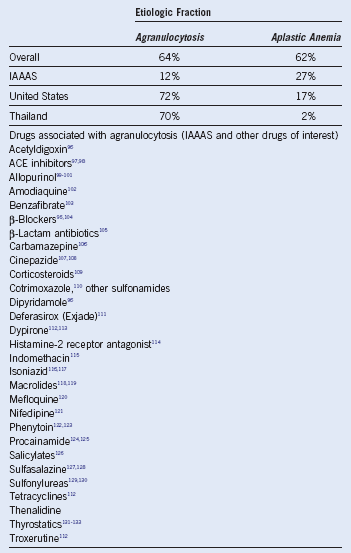
ACE, Angiotensin-converting enzyme; IAAAS, International Agranulocytosis and Aplastic Anemia Study.
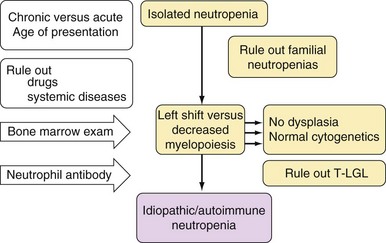
Table 6-4 Immunophenotype and Laboratory Features of T-Cell Large Granular Lymphocyte Leukemia
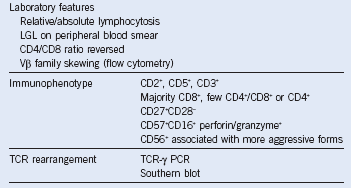
LGL, Large granular lymphocyte; PCR, polymerase chain reaction; TCR, T-cell receptor.
Approach to the Diagnosis and Treatment of Acquired Pure Red Cell Aplasia, Acquired Neutropenia, and T-Cell Large Granular Lymphocyte Leukemia
Related posts:
 Heme Biosynthesis and Its Disorders: Sideroblastic Anemia
Heme Biosynthesis and Its Disorders: Sideroblastic Anemia
 Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 2
Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 2
 Thrombotic Thrombocytopenic Purpura and the Hemolytic Uremic Syndrome
Thrombotic Thrombocytopenic Purpura and the Hemolytic Uremic Syndrome
 Hematology in Aging
Hematology in Aging
 Disorders of Phagocyte Function
Disorders of Phagocyte Function
 Inherited Forms of Bone Marrow Failure
Inherited Forms of Bone Marrow Failure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


